



Why Don't Our Shoulders Subluxate?
by Martin Krause (1986 & 1996 & 2003)
Taber's cyclopedic medical dictionary describes subluxation as a partial or incomplete dislocation (p.1384). The shoulder provides a unique opportunity to examine joint stability and hence resistance to subluxation from an aspect of neuromuscular co-ordination as the shoulder has little other anatomical constraints to prevent subluxation. To stabilise the shoulder the humeral head (ball) needs to be kept closely applied to the surface of the glenoid (socket) and in such a fashion that it is not allowed to slip or lose position when force is applied during hand placement.
The upper extremity serves as an instrument to place the hand in a position of function (Rothman, Maverl, Heppenstall 1975). Perry (1978) noted that a person can accurately differentiate one degree of motion which means that in the glenohumeral joint with an average of 150 degrees of flexion and 30 degrees of extension, 180 distinct positions to differentiate exist in the sagital plane. If this is combined with 90 degrees of abduction then 16,000 distinct positions are possible. The addition of 50 degrees of rotation further increases the potential for the number of selected hand positions which need to be differentiated ( Turvey, Fitch, Tuller 1982) for joint stability (Rothman et al 1975).
In contrast to the hip, the shoulder appears to have little bony stability. The humeral head is inclined 130-150 degrees relative to the shaft, and retroverted an average of 20 degrees relative to the distal end of the humerus (Sarrafian 1983). The humeral articular surface represents approximately 1/3 of an irregular sphere (Cailliet 1980) with an average vertical dimension of the surface being 48mm, and a 25mm radius of curvature; the average transverse dimension is 45mm, with a 22mm radius of curvature (Sarrafian 1983). However, the oval glenoid surface has an average vertical dimension of 35mm, and a tranverse diameter of only 25mm (Sarrafian 1983). The concave and rather flat glenoid surface is approximately 1/4 the size of the convex humeral head, and hence little element of stability is provided by their fit (Sarrafian 1983, Cailliet 1980). Radiographic investigations reveal no anatomical differences between normal shoulders and those which recurrently subluxate (Paavolainen, Magnus, Bjorkenheim, Ahovuo, Slatus 1984; Cyprien, Vasey, Burdet, Bonvin, Kritsikis, Vuagnat 1983). Unfortunately, the attachment of the glenoid labrum does not substantially increase the depth of the concave surface (Sarrafian 1983), however its detachment has been referred to as the 'essential lesion' leading to recurrent anterior subluxations (Bankart 1938, Paavolainen et al 1984). Thus the shoulder possesses little bony stability required for hand placement.
The ligaments of glenohumeral joint also appear to provide little stability for the shoulder. The superior segment of the glenohumeral capsule and the coracohumeral ligament contribute to the vertical stability of the humeral head (Sarrafian 1983, Turkel, Panio, Marshall, Girgis 1981). The contribution of the anterior capsulo-ligamentous complex to the anterior stability of the humeral head is limited. The anterior, middle and inferior glenohumeral ligaments are mere thickenings of the capsule. Furthermore, a foramen of variable size, the foramen ovale of Weitbrecht, is present between the superior and the middle glenohumeral ligaments (Sarrafian 1983; Cailliet 1980). The inferior glenohumeral ligament is the largest and strongest of the three glenohumeral ligaments with its location between the subscapularis and teres minor tendons, reinforcing the inferior glenohumeral capsule (Sarrafian 1983). This anatomical feature is significant in that beyond 90 degrees abduction, the subscapularis tendon no longer provides anterior stability of the humeral head (Cailliet 1980; Baleman 1978; Kummel 1979; Turkel et al 1981; Paarvolainen et al 1984) so that the anterior stability must be provided by the axillary pouch of the inferior glenohumeral ligament (Turkel et al 1981; Sarrafian 1983; Ovesen and Nielsen 1985; Cailliat 1980; McGlynn and Caspari 1984).
The posterior stability of the humeral head is provided by the tendons of the infraspinatus and teres minor (Baleman 1978; Cailliet 1980). Sarrafian (1983) described these tendons as 'true active ligaments'. Together with the long head of biceps and the subscapularis, the teres minor and infraspinatus provide a dynamic anterior-posterior stability required for glenohumeral function and hence hand-placement (Burkhart 1991). Further, for superior-inferior stability, the deltoid contraction must be matched by teres minor, infraspinatus and subscapularis contraction (Burkhart 1991). In fact the infraspinatus, teres minor, and subscapularis are each thought to cover 3/10 of the capsule with the remaining 1/10 covered by the long head of biceps (Watson 1985). Tears of the rotator cuff tendons revealed three kinematic patterns of movement abnormalities which included "stable fulcrum kinematics" associated with tears of the supraspinatus (and part of the infraspinatus), "unstable fulcrum kinematics" associated with massive tears involving virtually all of the superior and posterior rotator cuff and "captured fulcrum kinematics" associated with massive tears of a major portion of the posterior rotator cuff and a major portion of the subscapularis resulting in an 'awning-effect' of the acromion (Burkhart 1992) . These investigations suggest that if any part of the antero-posterior stability is affected then at the very least an "impingement syndrome" "painful arc" may result.
Also important to consider is the movement of the scapular which acts to maintain a position of stability for the glenohumeral joint by orienting the glenoid so that contraction of the rotator cuff muscles results in compression of the humerus against the glenoid during activities involving arm elevation. Saha's (1983) analysis of scapulo-humeral movement was considered in three phases :
Phase I involves elevation to 60 degrees flexion or to 30 degrees abduction by
-
elevation of the outer end of the clavicle by approximately 12-15 degrees.
-
scapular rotation in an antero-posterior axis taking place in an irregular direction termed the "setting phase of the scapula".
-
increasing the angle between the scapula spine and clavicle by about 10 degrees through a counter-clockwise rotation of the scapula around a vertical axis through the acromioclavicular joint.
Phase II involves elevation from the end of phase I to 90 degrees flexion or abduction through
-
further elevation of the outer end of the clavicle to its final position (i.e. 30-36 degrees over its usual bearing with the midsagittal plane).
-
no change in the spino-clavicular angle
-
scapular rotation in the antero-posterior axis
-
no rotation of the clavicle in its long axis
Phase III encompasses elevation vertically overhead from the end of phase II position
-
no further elevation of the clavicle
-
a second quota of rotation of the scapula around the vertical by about 10 degrees
-
clavicular rotation in a 'crankshaft' fashion, with the glenoid tubercle pointing downwards through about 30-40 degrees
-
external rotation of the humerus as is necessary for elevation in the coronal plane.
Three dimensional acromioclavicular joint motions during elevation of the arm (Teece et al J Orthop Sports Phys Ther, 38(4), 181-90). During active scapula plan abduction from rest to 90 degrees, average A/C joint angular values demonstrated increased internal rotation (4.3 degrees), increased upward rotation (14.6 degrees), and increased posterior tilting (6.7 degrees).
Scapulohumeral rotation was considered to be an average of a 2:1 ratio for abduction.
Poppen and Walker (1976) found the centre of rotation of the glenohumeral joint, for abduction in the plane of the scapula, to be located within 6mm of the geometric centre of the humeral ball. The average excursion of the humeral ball in the face of the glenoid in the superior-inferior plane between each 30 degree arc of motion was less than 1.5mm in normal subjects. With this constraint of motion in mind, the theoretical construct of Saha (1983) may be examined.
If the glenoid cavity can be considered as a part of a sphere having its centre at G and radius R, and if the articular surface of the humerus is part of the surface of a smaller sphere with its centre at O and radius r then the following calculations may be constructed (see fig 1). 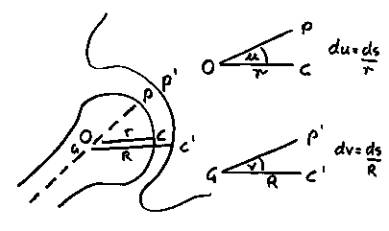
Figure 1. Glenohumeral coordinates.
In every position of the head, the point of contact C and the centres O and G are co-linear. Letting the centre of gravity of the limb act at m, the line m and O is the axis of the limb and when produced meets the articular surface at P. Therefore for different positions of the limb in a plane of the paper, angles POC and PGC will vary.
Letting the two angles in a particular position be u and V with the constant lines PO and PG respectively, then a rotation over a small surface (in the plane of the paper ds, in an instant dt) would be represented by
du = ds /r and dV = ds /R
so that the respective displacements are
du/dt = 1/r x ds/dt 1
dV/dt = 1/R x ds/dt 2
1 - 2
du/dV x R/ r
du = R/r x dV
u = R/r .V + k 3
however when P becomes the contact point C, then u = 0, v = 0
therefore the value K becomes zero, thus 3 reduces to
u = R/r .V 4
(Saha 1983, p7).
Now equation 4 states that even if the glenoid was stationary when there was a counter-clockwise rotation of the limb around O, there would occur counter-clockwise rotation of the head around G, but to a smaller extent (since r is less than R). So the head rolls to a new position governed by the equation (Saha 1983). Since the shortest distance from one point to another on an ovoid surface is a cord, and the shortest displacement is a cardinal displacement, then when two cardinal displacements follow each other at 90 degrees then spin or axial rotation must be introduced (Sarrafian 1983). Rolling movements are more economical to form than sliding or gliding movements thereby the ball rolls to minimise shear between the faces (Saha 1983) thereby attaining greater stability (Sarrafian 1983).
Saha (1983) believes that every position of the glenoid can be studied from two aspects
-
forces which bring the arm to a new position
-
forces which are responsible for fixation in a particular position
The humeral head contacts the glenoid at the point C. Thus COG is the direction of reaction due to contact, assuming after P1, P2, etc, the different pulls of muscles have brought the limb to a given position. With weight W acting at the centre of gravity M somewhere beyond the upper 1/3 of the forearm, the force at P1, P2, etc and W acting on the humerus cannot be in equilibrium because C is not a fixed fulcrum, neither is enough reaction resistance available to compress the head at C thus making the humerus liable to glide down on the glenoid without the intervention of other forces using the formula of equilibrium

where (alpha) a 1, a 2, a 3, etc are the angle at which the muscles pull at the limb whereas (beta) b is the angle made by the direction of weight with respect to the axis of rotation. Thus the compressive action of the infraspinatus, teres minor, and subscapularis are necessary to increase the reaction at the point of contact (P1,P2,etc) to hold the head against the glenoid (Baleman 1978; Cailliet 1980; Saha 1983) . The resulting acting forces are maximum at 90 degrees of elevation where shear and compression forces are equal (Post, Silver, Singh 1983), whereas the maximum shear forces occur at 60 degrees of abduction (Poppen et al 1978).
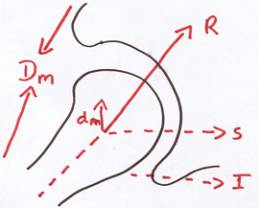
Figure 2 : Muscular reactive forces to the pull of deltoid.
Contraction of the deltoid alone (whilst in the neutral position) results in vertical shear of the head with respect to the glenoid and unless the head is rotated, depressed and compressed by the rotator cuff muscles the deltoid loses the power required during abduction (Baleman 1980; Neviasser 1980) . If the rotator cuff function is impaired even slightly then the normal fulcrum at C will be lost and abnormal translation (Subluxation) will result (Cailliet 1980). It is probable that if one force component of the rotator cuff is compromised then greater tension is exerted in the remaining rotator cuff muscles resulting in shear and compression of muscle capillaries with concomitant hypoxic damage to collagen fibres (Poppen et al 1976; Post et al 1983). Indeed "impingement syndrome" has been associated with posterior capsular tightness and a relative weakness of the external rotators and that anterior instability is associated with excessive external rotation and weakness of the internal rotators of the shoulder (Warner, Micheli, Arslanian, Kennedy, Kennedy 1990).
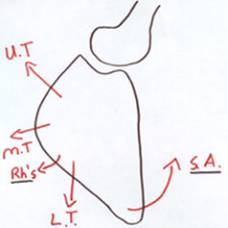
Importantly, for complete abduction, external rotation is required to allow the greater tuberosity to pass posterior to the acromial process and coracoacromial ligamentous arch (Cailliet 1980; Sarrafian 1983; Schenkman, de Cartaya 1987). Furthermore, scapula rotation is also required to provide efficiency of contraction (line of pull) to the rotator cuff and hence deltoid muscles (see fig.3) (Cailliet 1980). Suspension of the scapula is accomplished by the clavicle acting as a strut compressing at its inner end against the sternoclavicular joint. The suspensory mechanism is both static and dynamic and under constant stress due to gravity. The suspensory ligaments include the acromioclavicular, coracoclavicular and sternoclavicular ligaments, whereas the suspensory muscles include trapezius, sternocleidomastoid and levator scapulae (Baleman 1978). Upper fibres of trapezius pull the scapula upward and inward, pivoting about the acromioclavicular (A/C) joint (Cailliet 1980). The middle fibres of trapezius stabilise the scapula whereas the lower fibre of trapezius pull the medial border of the scapula down and hence rotate the glenoid up (Cailliet 1980). In association with the serratus anterior the upper and lower fibres of trapezius pivot the scapula about the A/C joint, thus elevating the glenoid fossa and contributing to scapulo-humeral rhythm (Cailliet 1980; Schenkman et al 1987).
Since only 30 degrees of clavicular elevation is permitted, corresponding to 30 degrees of scapula rotation, further elevation of the clavicle is checked by the costoclavicular and coracoclavicular ligaments which act as a force couple to cause the clavicle to rotate backwards around its long axis in a "crankshaft" effect resulting in a further 30 degrees of clavicular elevation (Schenkman et al 1987 ). Loss of this motion would prevent the shift of the axis of rotation from the sternoclavicular joint to the A/C joint and hence would prevent the lower fibres of trapezius and lower digitations of serratus anterior to function as an upward rotator (Schenkman et al 1987). Furthermore, the rhomboids elevate the medial aspect of the scapula thereby causing downward rotation of the glenoid fossa and hence may create instability at the glenohumeral joint (see fig. 4). If the glenoid does not move upward during abduction then the line of pull of the rotator cuff may result in excessive translation and hence glenohumeral instability since the attachment of the rotator cuff to the scapula will mean that they are dependent upon appropriate positioning of the scapula for glenohumeral stability.
 |
 |
| Figure 3 : Lines of action of scapula and rotator cuff muscles. | |
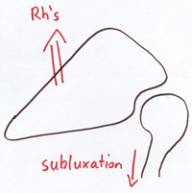
Figure 4 : Line of action of the rhomboid muscles and glenohumeral instability.
The previous discussion highlights that scapulohumeral rhythm comprises of a number of relative independent muscles constrained to act as a unit to provide glenohumeral stability (Turvey, Shaw, Mace 1978; Turvey, Fitch, Tuller 1982). With such a vast number of combinations of degrees of freedom the question of neuromuscular control needs to be addressed (Bernstein 1967; Perry 1978; Turvey et al 1982). Context-conditioned variability as a fixed relationship cannot be assumed between muscle states and movement ( Turvey et al 1982) and it is the contextual setting which distinguishes 'actions' from movements (Glencross 1980; Turvey et al 1978; Whiting 1980). Nociceptive input from inflammatory substances such as bradykinin, potassium, prostaglandin and serotonin (Cairns 2007), accumulation of calcium and anaerobic metabolites (Rosendal et al 2004) interact with the function of spinal cord interneurones and motor neurones (Madelaine 2008). Together with a general inhibitory effect of nociception on agonist and antagonist gamma motoneuron proprioceptive function (Mense & Skepper 1991) suggests that any variation in muscle tone (resting electrical activity) due to reflexogenic muscle spasm from inflammation, or weakness from nerve compression may compromise the stability at the glenohumeral joint and thus constrain the number of possible 'actions'.
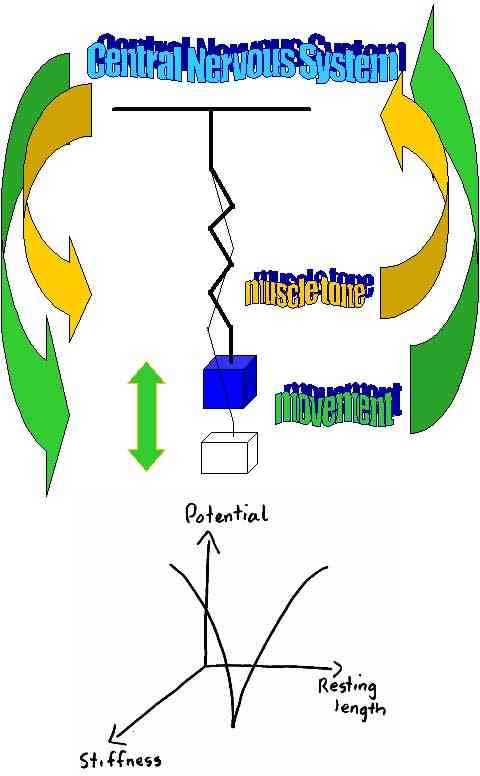
A "mass-spring" analogy has been generated which would dictate that no matter from which position a limb started it would maintain neuromuscular control by adjusting automatically to changes in context (Turvey et al 1982). This means that the total amount of motoneuronal activity is adjusted to the demands of function (speed, range of movement, weight) through higher centre modulation of electrical activity to all the muscles of the scapulohumeral complex. The only stability for a non-linear system whose processes degrade large amounts of free energy is a dynamic stability consisting of periodicities or cycles (Kugler, Kelso, Turvey 1980). This mechanical hypothesis is very attractive as the central nervous system appears to modulate in periodicities or cycles (Segundo, Stiber, Vibert, Hanneton 1995; Segundo, Vibert, Stiber, Hanneton 1995).
M X + KX + SX = F(t)
M=mass K=friction coefficient S=stiffness coefficient X=displacement F(t)=force function
Neural and mechanical variables in dynamic stability
Non-linear cycles have a tendency to a fixed amplitude and frequency no matter how disturbed, a tendency not to increase in amplitude when driven at their preferred frequency, and a tendency to mutually entrain or synchronize (Kugler et al 1980). Langley and Zelaznik (1984) suggest that the variables pertinent to a particular motor task can be divided into two classes
a) essential variables which determine the structure or topographic characteristics of the motor output, and therefore coordination and,
b) non-essential variables whose values can change in a scaled manner while leaving the basic movement structure in tact (Kugler et al 1980; Kelso, Putnam, Goodman 1983; Kelso, Southard, Goodman 1979; Turvey et al 1978) . See sitting vs standing cycling kinemtics at the knee elsewhere on this site , where the hamstring, quadriceps and gluteal muscles may provide powerful extension of the knee during pedalling of a bicycle. Similar, oscillatory control can be seen in the foot orthotic section of this website, where the pronation-supination of the foot and tibial oscillation at the knee provide an example of dynamic stability.
An inflection point identifies a stable configuration of the system's dimensions, i.e. a point about which the dimensions will tend to configure to subsequent perturbations. The geometric profile exhibits an inflection region at the resting length with ascending gradients on both sides. Distances may be regulated through the manipulation of the resting length while velocity and acceleration may be regulated through the manipulation of stiffness (see fig. 5) (Kugler et al 1980). Stiffness and the variable "resting length" corresponds to the selection of firing rate (Kelso 1982). Importantly, extrapolation of the inflection point to the clinical setting may mean that the 'setting phase' is critical to the correct implementation of movement.
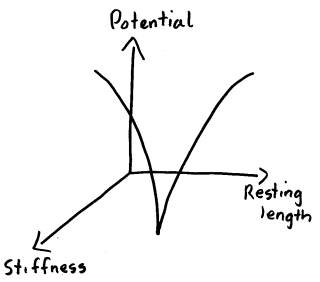 Figure 5 : Geometric variables of the "mass-spring" analogy
Figure 5 : Geometric variables of the "mass-spring" analogy
Importantly, in the clinical setting there will be several aspects of movement control to consider. Essentially, in the early phase of rehabilitation the pain and inflammation need to be reduced to provide the optimal interneuronal pool firing. Additionally, through the reduction of pain the cognitive focus can be on achieving the stabilising inflection point and gradually building the movement repertoire based on managing the control of the newly attained degrees of freedom. Thus, early rehabilitation uses 'closed kinetic' chain exercises where the hand is fixed to an immobile object e.g. the floor or the wall, whereas later rehabilitation uses 'open kinetic' chain visual cues to manage the degrees of freedom. This would involve higher centre calculations of trajectories and timing of impact which manipulate acceleration and deceleration variables. Clinically these later stages of rehabilitation may find that useful visual cues could involve the use of markers on walls or possibly even children's interactive computer gaming such as the Sony Wiifit.
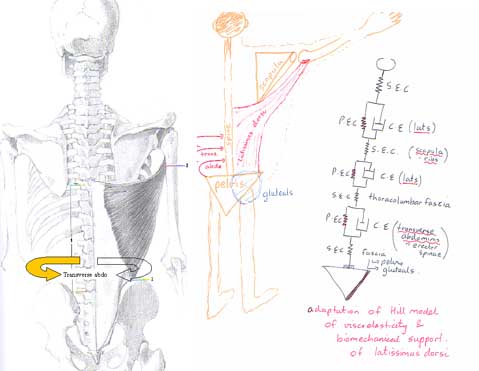
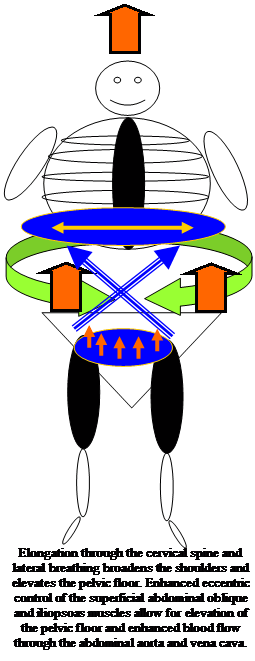
Frequently, the emphasis of closed kinetic chain exercises is to enhance scapula mobility and stability to enable the optimal positioning of the glenoid fossa for the head of humerus. This approach also attempts to improve kinesthesia of the scapula which is frequently disrupted either due to pain and/or lack of visually reinforced input. The inflection points of stability for the scapula are highly likely to involve the interaction of the serratus anterior. For example, during the phase beyond 30 degrees of abduction, the emphasis would be on stability around the superior angle of the scapula (using upper serratus anterior, levator scapula, upper and middle trapezius and subclavius muscle tone) whilst the inferior angle maintains a forward and upward trajectory along the the thorax based on the muscle tone of the inferior serratus anterior, the latissimus dorsi (which attaches to the inferior angle) and the intercostal muscles which control the excursion of the ribs. In later phases of abduction where the axis of rotation resides at the A/C joint then interaction with descending fibres of the trapezius muscle tone increases in importance.
Since fibres of the serratus anterior blend with the external oblique, in addition to the latissimus dorsi attaching to the transverse abdominis and pelvis, the importance of abdominal stability and lumbo-pelvic control cannot be ignored when rehabilitating the shoulder. One need look no further than the big buttocks of tennis players to see how important the gluteal and trunk muscles are for controlling torques during the serving action. Therefore, the concept of providing joint stability through afferent-efferent equilibrium under higher centre control may be applied not only to the shoulder but also to every other joint in that particular synergistic movement. The simple arm action of small fast flexion-extension around 90 degrees flexion can be felt in the on-off action of the contralateral lumbar paraspinal muscles. The concept of abdominal-paraspinal muscles stabilising the lumbar spine and interacting with arm movement have been investigated (Richardson, Jull, Toppenburg, Comerford, 1995; Richardson, Toppenburg, Jull, 1995) .
Importantly, oscillations in another part of the body can be used to establish harmonic frequency elsewhere. For example, arm movements activating the opposite erector spinae activity, pelvic oscillations for scapular control, arm lifts for contra-lateral gluteal activity.

Alternate kneading of the hands into something soft activates the abdominal muscles, spinal rotatores and scapula muscles. Oscillations of the pelvis around the hip activates eccentric scapula control.
Alternate lifting of the arm off the wall activates the opposite buttock muscle.

Alternating arm flexion/extension around the 90 degree angle activates the opposite erector spinae muscles of the low thorax and upper lumbar spine. Moving through the horizontal with a consistent oscillation also has varying effects on those muscles.
Importantly, if loading is required to activate a muscle building response, then repetitions need to include tremor. Either fine motor tremor or exhaustion tremor, if we want to include a 'deterministic chaotic variable', which it is hypothesised to create an immune training variable. Interested readers, on chaos, should view https://www.back-in-business-physiotherapy.com/health-advocacy/exercise-and-the-immune-system-during-covid-19.html
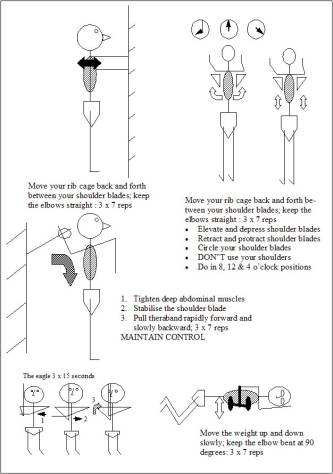
Figure 6: closed and open kinetic chain exercises.
The "meaning" of a descending "command signal" is significantly affected by the state of the spinal interneural pools into which it is sent. Nashner and Cordo (1981) demonstrated that the latency to firing, the intensity of activity, and coordination amongst different muscles all varied according to whether the muscle was functioning as a postural stabilizer, or was a prime synergist involved in a movement. Postures, like movements, are not triggered by stimulation, but are functional organizations of supporting musculature, capable of adaptation to changing circumstances (Kelso, Putman, Goodman 1983; Nashner 1976; Reed 1982) . Where a collective of muscles functions as a unit, the efferent-afferent distinction becomes superfluous where information about the given state of a muscle is by virtue of the linkage a specification of the states of the other muscles (efference) to which it is functionally linked (Kelso et al 1980; Kugler et al 1980) . Unfortunately, if afferent input is increased due to pain then excessive efferent activity may result (Gracely, Lynch, Bennett 1992; Woolf 1983; Woolf, Shortland, Sivilotti 1994; Woolf & Swett 1984). Due to a mismatch between 'efference copy' and afferent input, dyskinesia at lower levels of neuronal processing could result. A pain adaptation model has been proposed whereby pain results in increased anatagonist and decreased agonist activity (Svensson 2008). Moreover, the deeper joint muscles have a high density of muscle spindles (Bakker & Richmond 1982) suggesting that nociceptive input can disrupt their proprioceptive stabilizing function (Pederson et al 1998, Johansson et al 1995). Furthermore, sympathetic nervous system can result in reflexogenic changes in muscle activity (Passatore & Roatta 2007) including reduced muscle spindle discharge inhibition (Grassi et al 1993). Furthermore, the mechanisms of release and reuptake of Ca ions from/into the sarcoplasmic reticulum and the activity of the Na/K pump across the sarcolemma bear importance in the development of muscle force and are affected by sympathetic activation (Bowman 1980). These changes, taken together have been shown to affect feed-forward mechanisms of shoulder-neck motor control (Falla et al 2004). Therefore, reduction in pain, improved proprioception and higher order cognitive processing through descending modulatory mechanisms are of paramount importance in the clinical setting when pain is present.
Thorax
Patients frequently seek treatment for pain in various parts of the body, but infrequently present for treatment of thoracic pain. Yet, simple, quick assessment and correction of the thoracic rings frequently demonstrates a link to the pain and musculoskeletal dysfunction in areas some distance away. Wainner et al (J orthop Sports Phys Ther, 2007; 37, 658-660) describe regional interdependence as “the concept that seemingly unrelated impairments in a remote anatomical region may contribute to, or be associated with, the patient’s primary complaint.” This perception suggests that interventions targeting adjacent anatomical areas may directly affect the outcomes of the involved joint. Boyles et al (Manual Therapy, 2009 Aug;14(4):375-80) and Strunce et al (J Man Manip Ther, 2009, 17(4): 230-236) have demonstrated the immediate effects of thoracic spine thrust manipulation on patients with shoulder impingement syndrome. The latter describing a 51% reduction in shoulder pain, 30-38 degree increase in range of motion (ROM), and a mean patient perceived global rating change of 4.2 in 21 subjects. McCormack (J Man Manip Ther., 2012 Feb;20(1):28-34) showed a 25 degree improvement in shoulder ROM when using thoracic spine manipulation in the treatment of adhesive capsulitis. Brian Mulligan described 'mobilisation with movement' (MWM) techniques on the first rib which have dramatic effects on the cervical ROM for contralateral lateral flexion and ipsilateral rotation. Canadian physiotherapist Linda Joy Lee has advocated ring shift corrections for low back pain, pelvic girdle pain and hip problems, as well as shoulder and neck issues.
Interested readers should look at the thorax aspect of this website.
Since an individual may perform a task at near maximal tolerance it is important that the muscular energy intended for the task (e.g. hitting a ball with a racquet) is not misdirected inwards and transferred to bone, ligaments, capsule, and nerve due to sudden unexpected perturbations of movement and/or pain and/or in-coordination (Jobe & Jobe 1983). Human tissue can hypertrophy and decrease the probability of injury. Also improved coordination and metabolic efficiency can be attained through an appropriate treatment regime (Astrand, Rhodal 1977; Jobe et al 1983; Sale, Macdougall 1981). Moreover, non-injurous activity results in the production of proteoglycans both in the joints and periarticular structures thereby increasing strength and flexibility of collagen (Jobe et al 1983). The general effect of appropriate long-term activity (hypertrophy, rehearsal, metabolic efficiency and flexibility) is referred to as "conditioning" (Jobe et al 1983). See the endurance training-plyometrics section elsewhere on this site.
During the rehabilitation of the shoulder the physiotherapist may need to appreciate the synergistic action of the large number of muscles acting around the shoulder. It may be important to decrease afferent input which is undesirable to efficient movement such as pain and excessive stiffness from cervical, thoracic, lumbar and shoulder structures. Therefore, joint mobilisations of the spine may play an important role in the treatment of the shoulder. Additionally, it would appear that optimal coordination will mean the use of functional, specific, pain-free movements perhaps with the aid of muscle stimulating or inhibiting tape, pain inhibitory tape and/or the use of elastic bands of varying resistance . During rehabilitation, attention to detail not only at the glenohumeral joint but also at the scapula should result in a functional stable shoulder which does not subluxate.
Ultimately, this optimisation of neural input and outputs can be seen in the relative fluidity and graciousness of expert performers versus the relative rigidity of the novice. The expert performer can chunk motor activity into object oriented subconscious anticipatory behaviour whereas the novice is still reliant on the slowness of several instances of feedback and the limited conscious level cognitive processing of short term memory.
Summary
- the rotator cuff muscles provide glenohumeral stability
- the scapular muscles provide the positioning for inferior stability of the glenoid labrum for a snug fitting humeral head
- with the deep joint stabilizing muscles providing the stability, the prime movers may provide the 'action'
- generally speaking the stabilizing muscles of most joints are one joint muscles with an endurance function; whereas the prime movers are the muscles which lend power to the movement e.g. Pectoralis Major. Therefore when designing an exercise regime the client must begin with good muscular stability before commencement of training of the prime movers.
- Frequently, clients compensate for lack of stability by increasing the speed at which they do the task. This then leads to further in-coordination, poor timing between muscles, loss of synergy, and more dysfunction.
- Closed kinetic chain training to gain scapula and rotator cuff stability may encourage gamma afferent feedback from the annulospiral endings, as well as activate the nuclear bag and nuclear chain fibres
- Plyometric type exercises using theraband are designed to encourage eccentric-concentric control of the prime movers.
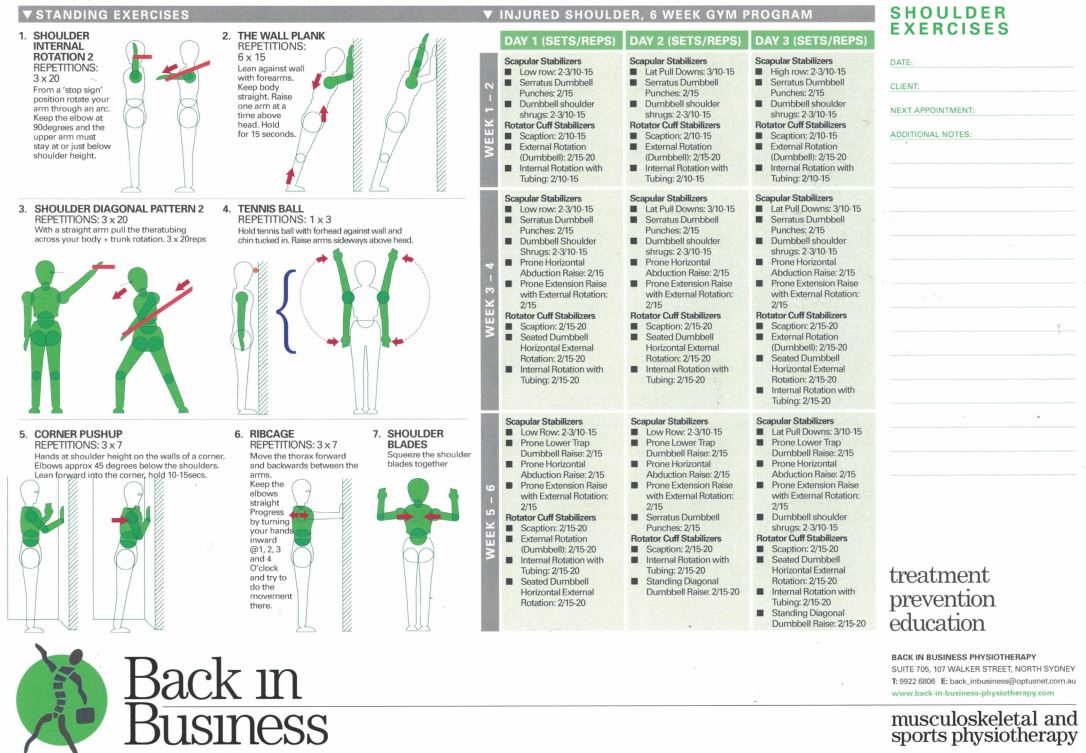
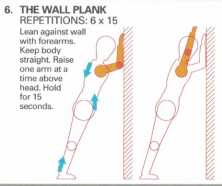
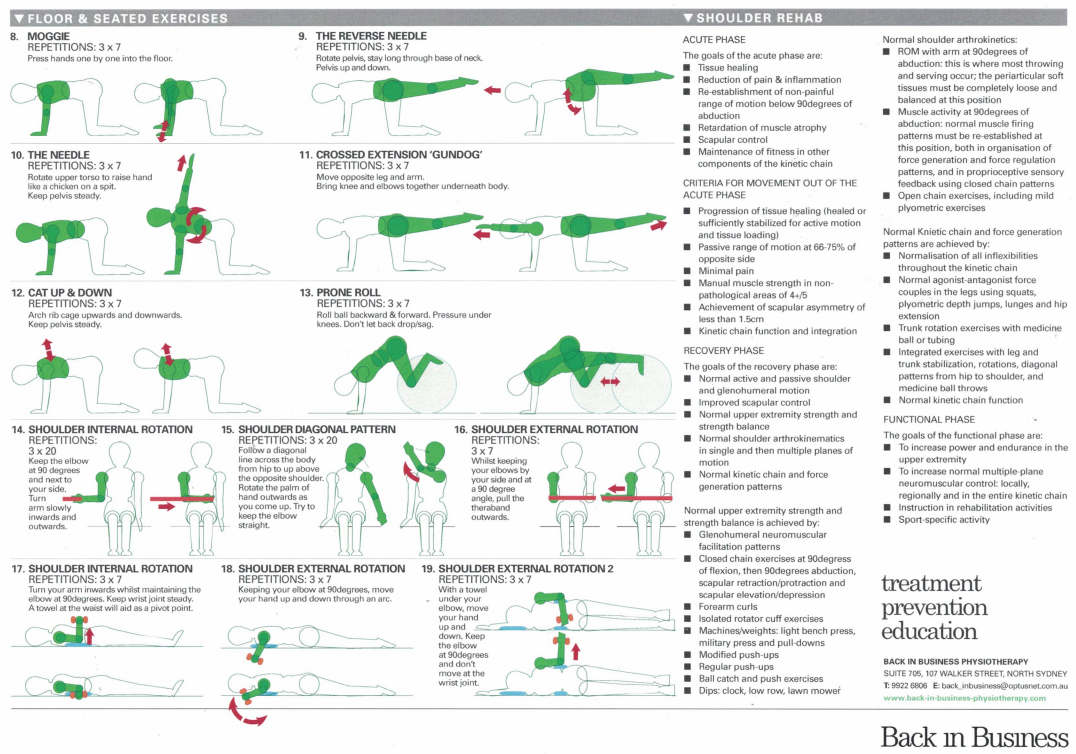
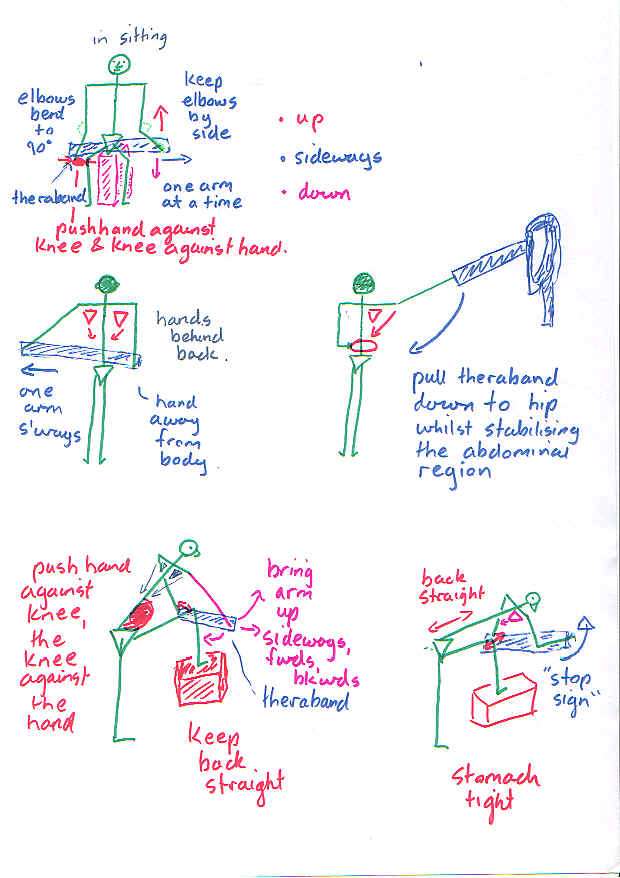
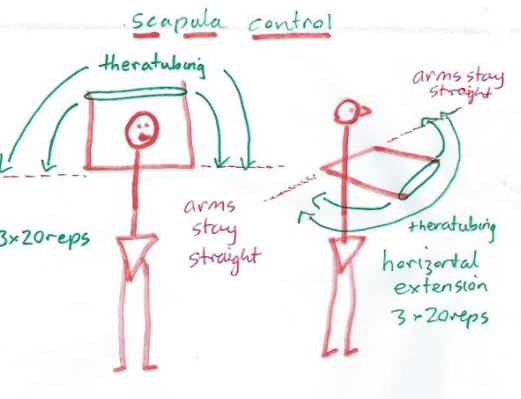
Closed kinetic chain exercises 5, 8-13, promoting stability. Should be done slowly, as the deep stabilising muscles are red slow twitch muscle fibres. Such exercises combine the shoulder, neck, shoulder blade, thorax and pelvic complex to functionally stabilizing activities. Moreover, Swiss Ball Exercises in 2 and 4 point Kneeling can be used to promote over-shoulder-height arm activity whilst having the arms below the shoulders!!! Apart from the Prone Roll, the Swiss Ball can also be used to do diagonal upward rolls as well as prone scissors. Open chain dynamic exercises can eventually be incorporated whilst kneeling on the Swiss Ball
Plyometrics - open kinetic chain
Open kinetic chain exercises are essentially less stable than closed kinetic chain exercises. They fall into two essential categories - those which pull inward and hence energy towards to body and those wish pull away. Basically, hypermobile people need to focus on stability, perfecting closed kinetic chain exercises, moving on to a hybrid of closed kinetic chain with open kinetic chain pulling inwards and eventually adding the open kinetic chain pulling outwards.
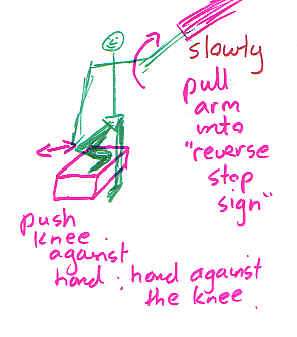
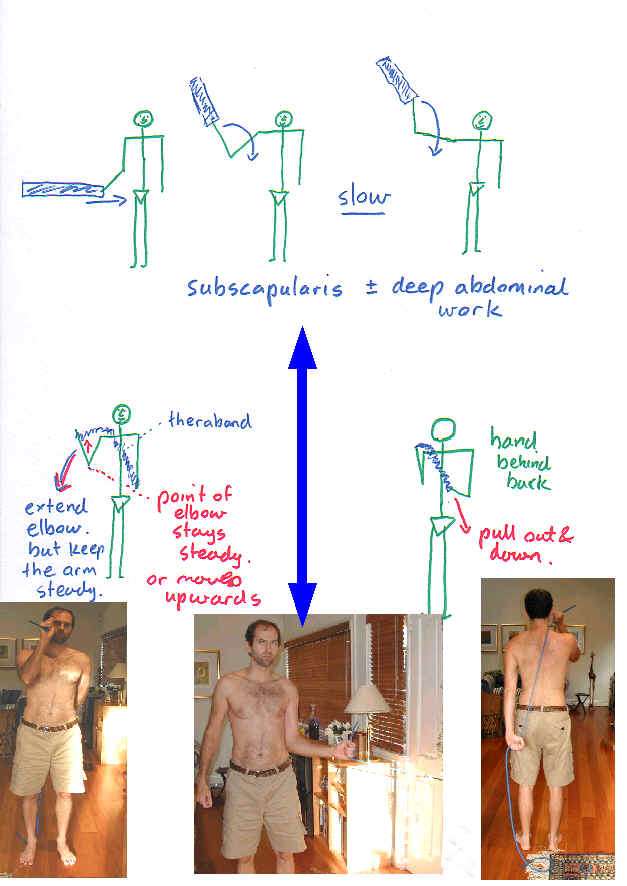
Care needs to be taken with the open kinetic chain internal and external rotation as it's not uncommon to aggravate the transverse ligament and long head of biceps with this exercise. Additionally it isn't a very functional exercise. Exercises that more closely mimic the activity to which the person needs to return to, will generally be more effective, as well as present an opportunity to use the exercise as a metric on the path to recovery.

EMG biofeedback
Altered immune responses and altered lipid metabolism have been implicated as a causative factor in shoulder tendinopathies. Interested readers should look at Exercise and the Immune System as well as Exercise and Weight Loss elsewhere on this website for further explanations.
Sodium Hyaluronate and Platlet Rich Plasma (PRP) for partial thickness rotator cuff tears
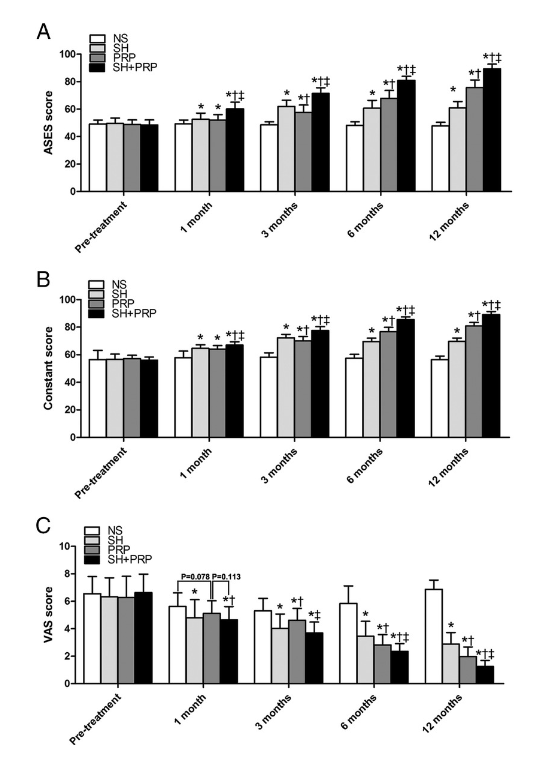
Investigations have demonstrated improvements in pain and function, in small to medium sized supraspinatus tendon tears, up to 12 months after PRP and Sodium Hyaluronate injections, in 45 people who received PRP injections and 48 people who had a combination of sodium hyaluronate and PRP injections (Cai et al 2019, Med sc Sp Ex, 51, 2, 227-233).
Interesting articles
these articles are particularly interesting in respect to synergistic 'timing' of muscle action in the upper and lower limbs
Commerford & Mottram (2001). Functional stability re-training: principles and strategies for managing mechanical dyfunction. Manual Therapy, 6,1, 3-14
Commerford & Mottram (2001). Movement and stability dysfunction - contemporary developments. Manual Therapy, 6,1, 15-26
Animated muscular synergistic interaction for shoulder abduction - refer to Climbing section
Shoulder Problems(English)
Schulter Probleme (Deutsch)
Original paper on motor control written by Martin Krause in 1986. Influencing factors of pain on muscle tone was added in 1996.
Visual variables and cognitive reasoning in motor control has been described by me elsewhere using orienteering as an example in 2003:
Scapular Rotation to Attain the Peak Shoulder External Rotation in Tennis Serve
KONDA, SHOJI; YANAI, TOSHIMASA; SAKURAI, SHINJI
Medicine & Science in Sports & Exercise. 42(9):1745-1753, September 2010.
Abstract:
Purpose: The purposes of this study were (a) to describe the detailed movements of the shoulder complex during the cocking phase in tennis serve and (b) to determine the contribution of the scapular rotation to the peak shoulder external rotation attained at the end of the cocking phase.
Method: Twenty tennis players performed flat tennis serves with the maximum effort, and three-dimensional kinematic data of the thorax, scapula, and humerus of the dominant side were recorded by an electromagnetic tracking device (Liberty; Polhemus) at 240 Hz. The humeral rotation with respect to the thorax (named as the resultant shoulder rotation) was decomposed into the scapular rotation with respect to the thorax and the humeral rotation with respect to the scapula (named as the glenohumeral rotation). The scapular rotation that contributed to attain the peak resultant shoulder external rotation was quantitatively determined, and the ratio of the glenohumeral external rotation to the scapular rotation that contributed to attain the peak resultant shoulder external rotation was computed to represent the scapulohumeral rhythm for shoulder external rotation.
Results: Of the three components of scapular rotations, the scapular posterior tilt was the primary component that contributed to the attainment of the peak resultant shoulder external rotation. The scapulohumeral rhythm for shoulder external rotation (scapular posterior tilt-glenohumeral external rotation) exhibited during the backswing phase was 1:2.3.
Conclusions: The peak resultant shoulder external rotation was generated by a synchronized combination of the scapular posterior tilt and glenohumeral external rotation. A consistent pattern of three phases of the scapular posterior tilt and the glenohumeral external rotation that could be accurately modeled by three linear regressions was observed in preparation for the peak shoulder external rotation in tennis serve.
The short-term effects of thoracic spine thrust manipulation on patients with shoulder impingement syndrome?
Robert E. Boyles, Bradley M. Ritland, Brian M. Miracle, Daniel M. Barclay, Mary S. Faul, Josef H. Moore, Shane L. Koppenhaver, Robert S. Wainnerc
Manual Therapy 2009, 14, 375-380
The study was an exploratory, one group pretest/post-test study, with the objective of investigating the short-term effects of thoracic spine thrust manipulations (TSTMs) on patients with shoulder impingement syndrome (SIS).
There is evidence that manual physical therapy that includes TSTM and non-thrust manipulation and exercise is effective for the treatment of patients with SIS. However, the relative contributions of specific manual therapy interventions are not known. To date, no published studies address the short-term effects of TSTM in the treatment of SIS.
Fifty-six patients (40 males, 16 females; mean age 31.2±8.9) with SIS underwent a standardized shoulder examination, immediately followed by TSTM techniques. Outcomes measured were the Numeric Pain and Rating Scale (NPRS) and the Shoulder Pain and Disability Index (SPADI), all collected at baseline and at a 48-h follow-up period. Additionally, the Global Rating of Change Scale (GRCS) was collected at 48-h follow-up to measure patient perceived change.
At 48-h follow-up, the NPRS change scores for Neer impingement sign, Hawkins impingement sign, resisted empty can, resisted external rotation, resisted internal rotation, and active abduction were all statistically significant (p<0.01). The reduction in the SPADI score was also statistically significant (p<0.001) and the mean GRCS score=1.4±2.5.
In conclusion, TSTM provided a statistically significant decrease in self reported pain measures and disability in patients with SIS at 48-h follow-up.
Motion analysis study of a scapular orientation exercise and subjects’ ability to learn the exercise
Sarah L. Mottram, Roger C. Woledge, Dylan Morrissey
Manual Therapy 2009, 14, 13-18
Exercises to retrain the orientation of the scapula are often used by physiotherapists to optimise shoulder girdle function. The movements and muscle activity required to assume this position have not yet been quantified. Further, patients often find this a difficult exercise to learn accurately, with no data being available on the accuracy of repeated performance. The primary objective of this study was to quantify the movements occurring during a commonly used scapular orientation exercise. The secondary objective was to describe the ability of subjects to learn this position after a brief period of instruction. A group of normal subjects (13 subjects; mean age 32, SD=9) were taught the scapular orientation exercise. Measurement of the position and muscle actions were made with a motion analysis system and surface electromyography. Further comparison was made of the accuracy of repeated trials. The most consistent movements were upward (mean=4°, SEM=0.9°) and posterior rotation (mean=4°, SEM=1.6°). All parts of the trapezius muscle demonstrated significant activity in maintaining the position while latissimus dorsi did not. Repeated trials showed that subjects were able to accurately repeat the movement without guidance. The key movements of, and immediate efficacy of a teaching approach for, scapular orientation have been established.
Mobilizations of the asymptomatic cervical spine can reduce signs of shoulder dysfunction in adults
Lynda McClatchie, Judi Laprade, Shelley Martin, Susan B. Jaglal, Denyse Richardson, Anne Agur
Manual Therapy, 2009, 14, 369-374
Generalized shoulder pain is a common problem that is difficult to treat and frequently recurrent. The asymptomatic cervical spine must be ruled out as a cause of any shoulder pain, as it can have a similar presentation to an isolated shoulder disorder. Previous studies have shown that lateral cervical glide mobilizations to the asymptomatic cervical spine at C5/6 can affect peripheral pain, but none have examined shoulder pain. A randomized, blinded, placebo-controlled, cross-over trial was used to examine the immediate effects of cervical lateral glide mobilizations on pain intensity and shoulder abduction painful arc in subjects with shoulder pain. Twenty-one subjects received interventions of both cervical mobilization and placebo over two sessions. Pain intensity using a visual analog scale (VAS) and painful arc were assessed prior to and following application of cervical mobilization or placebo intervention. Evaluation of cervical mobilization revealed the shoulder abduction painful arc (12.5° ± 15.6°, p = 0.002) and shoulder pain intensity (1.3 ± 1.1 cm, p < 0.001) were significantly decreased. The results of this study suggest that any immediate change in shoulder pain or active shoulder range of motion following cervical mobilizations indicate that treatment directed toward the asymptomatic cervical spine may expedite recovery.
The initial effects of a Mulligan's mobilization with movement technique on range of movement and pressure pain threshold in pain-limited shoulders
Pamela Teys, Leanne Bisset, Bill Vicenzino
Manual Therapy, 2008, 13, 37 to 42
There is little known about the specific manual therapy techniques used to treat painfully limited shoulders and their effects on range of movement (ROM) and pressure pain threshold (PPT). The objective of this study was to investigate the initial effects of a Mulligan's mobilization with movement (MWM) technique on shoulder ROM in the plane of the scapula and PPT in participants with anterior shoulder pain. A repeated measures, double-blind randomized-controlled trial with a crossover design was conducted with 24 subjects (11 males and 13 females). ROM and PPT were measured before and after the application of MWM, sham and control conditions. Significant and clinically meaningful improvements in both ROM (15.3%, F (2,46)=16.31 P=0.00) and PPT (20.2%, F(2,46)=3.44, P=0.04) occurred immediately after post treatment. The results indicate that this specific manual therapy treatment has an immediate positive effect on both ROM and pain in subjects with painful limitation of shoulder movement. Further study is needed to evaluate the duration of such effects and the mechanism by which this occurs.
In 2011 Dr George Murrell and Dr Stephen O'Brien described references to altered lipid metabolism and altered immune activity in the form of cytokines occuring in tendonopathy. It has been shown that regular resistance training and/or endurance exercise attenuates altered immune responses. Interested readers should have a look at immune systems and obesity elsewhere on this website.
References
Astrand, P.O., Rodahl, K., (1977). Textbook of Work Physiology (2nd ed). McGraw Hill. New York .
Baleman, J.E., (1977). The Shoulder and Neck (Chapter 3). W.B. Saunders. Philadelphia .
Bakker & Richmond (1982). Muscle spindle complexes in muscles around the upper cervical vertebrae in the cat. J. Neurophysiol, 48, 62 to 74
Bankart, A.S.B., (1938). The pathology and treatment of recurrent dislocation of the shoulder joint. British Journal of Surgery , 26 , 23 to 29.
Bernstein NA (1967). The Co-ordination and Regulation of Movements, ch. II & IV. Pergamon Press, Oxford.
Bowman WC (1980) Effects of adrenergic activators and inhibitors on skeletal muscles. In Szekeres L (Ed) Adrenergic activators and inhibitors. Handbook of Experimental Pharmacology, 54, pp47 to 128, Springer Verlag, New York.
Burkhart, S.,S. (1991). Arthroscopic treatment of massive rotator cuff tears : Clinical results and biomechanical rationale. Clinical Orthopaedics and Related Research , 267 , 45 to 56.
Burkhart, S.,S. (1992). Fluoroscopic comparison of kinematic patterns in massive rotator cuff tears : a suspension bridge model. Clinical Orthopaedics and Related Research , 284 , 144 to 152.
Cailliet, R., (1980). The Shoulder in Hemiplegia . E.A. Davis Co. Philadelphia .
Cairns BE (2007) Physiological properties of thin-fiber muscle afferents: excitation and modulatory effects. In Fundamentals of Musculoskeletal Pain, Graven-Nielsen & Arendt-Nielsen & Mense Eds, IASP Press Seattle
Falla et al (2004) Feedforward activity of the cervical flexor muscles during voluntary arm movements is delayed in chronic neck pain. Exp Brain Res, 157, 43 to 48
Johansson et al (1995). A method for analysis of encoding of stimulus separation in ensembles of afferents. J Neurosci Methods, 63, 67 to 74
Glencross, D.J., (1980). Levels and strategies of response organizations. In : Stelmach, G.e., Requin, J., (Eds). Tutorials in Motor Behavior . Nth. Holland Pub. Co. .
Gracely, R.H., Lynch, S.L., Bennett, G.J., (1992). Painful neuropathy : Altered central processing maintained dynamically by peripheral input. Pain , 51 , 175 to 194.
Grassi C et al (1993) Modulation of the jaw jerk reflex by the sympathetic nervous system. Arch Ital Biol, 131, 213 to 226
Grassi C et al (1993) Effect of sympathetic nervous system activation on the tonic vibratory reflex in rabbit jaw closing muscles. J Physiol, 469, 601 to 613
Kelso, J.A.S., (1982). Part 1 : Perspectives and issues in motor behavior. In ; Kelso, J.A.S (Ed). The Process Approach to Understanding Human Motor Behavior : an Introduction . Erlbaum. New York .
Kelso, J.A.S., Putman , C.A. , Goodman, D., (1983). On the space-time structure of human interlimb co-ordination. Quarterly Journal of Experimental Psychology , 35A , 347to 375.
Kelso, J.A.S., Southard, D., Goodman, D., (1979). On programming and coordinating two handed movements. Journal of Experimental Psychology : Human Perception and Performance , 5 , 229 to 238.
Kuglar, P.N., Kelso, J.A.S., Turvey, M.T., (1980). On the concept of coordinated structures as dissipative structures. I : Theoretical lines of converged tutorials in motor behavior. p3 to 45. II : Emperical lines of convergence. pp 49-70. In : Stelmach, G.E., Requin, J., (Eds). Tutorials in Motor Behavior . Nth Holland Publ. Co. pp3 to 45.
Langley , D.J., Zelaznik, H.N., (1984). The aquisition of time properties associated with sequential motor skill. Journal of Motor Behavior , 16 , 3, 275 to 301.
Madelaine P (2008) Functional adpatations in work-related pain conditions. In Fundamentals of Musculoskeletal Pain, Graven-Nielsen & Arendt-Nielsen Eds, IASP Press Seattle Ch 25
Mense S & Skepper P (1991) Discharge behaviour of feline gamma-motoneurons following induction of an artificial myositis. Pain, 46, 201 to 210
McGlynn, F.J., Caspari, R.B., (1984). Arthroscopic findings in the subluxating shoulder. Clinical Orthopedics and Related Research , 183 , 3, 173 to 178.
Nashner, L.M., Cordo, P.J., (1981). Relation of automatic postural responses and reaction time of voluntary movements of human leg muscles. Experimental Brain Research , 43 , 395 to 405.
Ovesen, J., Nielsen, S., (1985). Stability of the shoulder joint. Acta Orthopaedica Scandinavia , 56 , 149 to 151.
Paavolainen, P., Bjoerkenheim, J.M., Ahovuo, J., Slaetis, P., (1984). Recurrent anterior dislocation of the shoulder. Acta Orthopaedica , 55 , 556 to 560.
Passatore et al (2007) Modulation operated by the sympathetic nervous system on jaw reflexes and masticatory movements. Arch Oral Biol, 52, 343 to 346
Pedersen et al (1998). Alterations in information transmission in ensembles of primary muscle spindle afferents after muscle fatigue in heteronymous muscle. Neuroscience, 84, 953 to 959
Perry, J., (1978). Normal upper extremity kinesiology. Physical Therapy , 58 , 3, 265 to 269.
Poppen, N.K., Walker, P.S., (1976). Normal and abnormal motion of the shoulder. The Journal of Joint and Bone Surgery , 58A , 2, 195 to 200.
Post, M., Silver, R., Singh, M., (1983). Rotator cuff tear. Clinical Orthopedics of North America , 173 , 3, 78 to 91.
Reed, E., (1982). An outline of a theory of action systems. Journal of Motor Behavior , 14 , 2, 98 to 134.
Richardson , C., Jull, G., Toppenburg, R., Comerford, M., (1995). Techniques for active lumbar stabilisation : A pilot study. Australian Journal of Physiotherapy Monograph, 1, 27 to 34.
Richardson, C., Toppenburg, R., Jull, G., (1995). An initial evaluation of eight abdominal exercises for their ability to prove stabilisation for the lumbar spine. Australian Journal of Physiotherapy Monograph , 1 , 21 to 26.
Rothman, R.H., Marvel, J.P., Heppenstall, R.B., (1975). Recurrent anterior dislocations of the shoulder. Orthopedic Clinics of North America , 6 , 2, 415 to 421.
Rosendal et al (2004) Increase in muscle nociceptive substances and anaerobic metabolism in patients with trapezius muscle myalgia: microdialysis in rest and during exercise. Pain, 112, 324 to 334
Saha, A.K., (1983). Mechanism of shoulder movements and aplea for the recognition of ?zero position? of the glenohumeral joint. Clinical Orthopedics and Related Research , 173 , 3, 4 to 10.
Sale , D., MacDougall, (1981). Sopecificity in strength training : a review for the coach and athlete. Canadian Journal of Applied Sports Medicine , 6 , 2, 87 to 92.
Sarrafian, S.K., (1983). Gross and functional anatomy of the shoulder. Clinical Orthopedics and Related Research , 173 , 3, 11 to 19.
Schenkman, M., de Cartaya, V.R., (1987). Kinesiology of the shoulder complex. The Journal of Orthopedic Sports Physical Therapy , 8 , 9, 438 to 450.
Segundo, J.P., Stiber, M., Vibert, J.F., Hanneton, S., (1995). Periodically modulated inhibition and its postsynaptic consequences - II. Influence of modulation slope, range, noise and of postsynaptic natural discharges. Neuroscience , 68 , 3, 693 to 719.
Segundo, J.P., Vibert, J.F., Stiber, M., Hanneton, S., (1995). Periodically modulation inhibition and its postsynaptic consequences - I. General features. Inluence of modulation frequency. Neuroscience , 68 , 3, 657 to 692.
Svensson P (2008) Pain and Jaw Motor Function. In Fundamentals of Musculoskeletal Pain, Graven-Nielsen & Arendt-Nielsen Eds, IASP Press Seattle, ch27
Tabers Cyclopedic Medical Dictionary .(1982) Clayton Thomas (Ed). F.A. Davis Co.. Philadelphia .
Townsend, H., Jobe, F.W., Pink, M., Perry, J., (1991). Electromyographic analysis of the glenohumeral muscles during a baseball rehabilitation program. American Journal of Sports Medicine , 19 , 3, 264 to 272.
Turkel, S.J., Panio, I.M.W., Marshall , J.L., Girgis, F.J., (1981). Stabilising mechanisms preventing anterior dislocation of the glenohumeral joint. The Journal of Bone and Joint Surgery , 63A , 8, 1208 to 1216.
Turvey, M.T., Fitch, H.L., Tuller, B., (1978). Part V : degrees of freedom, co-ordinative structure s and tuning. In : Kelso, J.A.S. (Ed). Human Motor Behavior : An introduction . Erlbaum. New Jersey .
Turvey, M.T., Shaw, R.E., Mace, W.M., (1978). Issues in the theory of action : Degrees of freedom, co-ordinative structures and coalitions. In : Requin, J., (Ed). Attention and Performance VII . (557 to 595). Erlbaum. New Jersey .
Turvey, M.T., Shaw, R.E., Reed, E.S., Mace, W.M., (1981). Ecological laws for perceiving and acting : A reply to Fodor and Pylyshyn. Cognition , 9 , 237 to 304.
Warner, J.J.P., Micheli, L.J., Arslanian, L.E., Kennedy, J., Kennedy, R., (1990). Patterns of flexibility and strength in normal shoulders and shoulders with instability and impingement. The American Journal of Sports Medicine , 18 , 4, 366 to 375.
Watson, M., (1985). Major ruptures of the rotator cuff. The results of surgical repair in 89 patients. The Journal of Bone and Joint Surgery , 67-B , 4, 618 to 624.
Whiting, H.T.A., (1980). Dimensions of control in motor learning. In : Stelmach, G.E., Requin, J., (Eds). Tutorials in Motor Behavior .(537-550). Nth Holland Pub. Co. .
Woolf, C.J., (1983). Evidence for a central component of post-injury pain hypersensitivity. Nature , 306 , 686 to 688.
Woolf, C.J., Shortland, P., Sivilotti, L.G., (1994). Sensitization of high mechanothreshold superficial dorsal horn and flexor motor neurones following chemosensitive primary afferent activation. Pain , 58 , 141 to 155.
Woolf, C.J., Swett, J.E., (1984). The cutaneous contribution to the hamstring flexor reflex in the rat : an electrophysiological and anatomical study. Brain Research , 303 , 299 to 312.
Last update : 4 November 2021
 What We do
What We do What We Treat
What We Treat



















































































































