



Existentialism
by Martin Krause
B.Appl.Sci. (Physiotherapy); M.Appl.Sci (Manipulative Physiotherapy), Post Grad Dip Hlth Sc (Exercise and Sports), Post Grad Cert Hlth Sc (Education)
Since the 1980's musculoskeletal physiotherapy has undergone extensive changes, originally based on a model of clinical outcomes with an unknown scientific rationale to one where the scientific rationale and evidence base over-rides the clinical reasoning based approach. This created an existential crisis amongst musculoskeletal physiotherapists whereby the discerning clinician began to validate their being against multiple and often competing 'gold standards' across not only their own profession but also against benchmarks which were set from without our profession, in the medical and other health profession domains. This resulted in a plethora of research amongst Musculoskeletal Physiotherapists employing theoretical and clinical models. The result was a profession which moved away from 'passive joint mobilisations' based on rudimentary biomechanical constructs, to a profession which employs multimodal treatments for the multiple dimensions of musculoskeletal dysfunction and pain. At back in Business Physiotherapy, these modalities still include joint mobilisations and manipulations, but now also encompass dry needling, muscle energy techniques, myofascial releases, 3 varieties of taping (Sports, Kinesio and Dynamic), neural mobilisations, thoracic ring relocations, and exercise regimes from all around the globe. Moreover, the tenate of the passive client receiving a passive treatment has been debunked by the research into motor learning and the immune and central nervous systems, which has demonstrated how important our explanations, empathy, and emotional understanding are in creating the trust needed for our human interactions. By considering the philisophical nature of this existential crisis, is it possible to understand how important it is to put the best interests of a healthy society at the forefront of every treatment intervention.
Index
- a Kafkaesque perspective on the role of physiotherapists and the Australian Physiotherapy Association
by Martin Krause, August 2004
In Franz Kafka's book 'The Trial', it outlined how a banker, Herr K, was notified that he was to stand trial. Throughout the book, the reader's frustration grows as Herr K refuses to attempt to defend himself, because he sees the trial as absurd as he doesn't know why he is being tried. Finally, he is condemned and we cannot understand why he didn't try to relate to his accusers. A misconception in language leading to a difference in ethics, morality, principles and hence reality? Existentialist philosophy believe that we can only be defined by our actions. Therefore, our responses to successes and failures will define us, and our insights can change the world.
Truth is considered a construct whereby reality cannot exist on it's own without reference to other information. Constructivism describes the process of learning and acquiring knowledge through experiential reasoning. The assumption underlying 'constructivism' is that we are 'life long learners' (3 l's) and that each and every clinical encounter allows a unique opportunity to learn, relearn and refine our techniques as well as reorganise and restructure our knowledge base. Furthermore, constructivist theory suggests that learning occurs which is based on each individuals unique prior experiences. Truth is considered relative to the individuals construct and hence diverges from logical positivism of science where 'truth' can exist alone without reference to the observers perceptions. This is similar to scientific philosophy of 'relative truths' or the 'relativity of knowledge' espoused by Feyerabend (1975), Kuhn (1970), Popper (1963). All of us would agree that science isn't just a collection of laws, or a catalogue of unrelated facts. Rather, it is a creation of the human mind relating to making sense of the world. Hence, in musculoskeletal physiotherapy we must endeavour to match the science with our clinical reasoning which should make sense to the individual or organisations with whom we are interacting. What we do is what defines us.
Candy (1991, p 263) states that "the constructivist perspective differs significantly from the view of knowledge as deriving from a process of copying or replicating." Hence, "we know reality only by acting on it.....The active interaction between the individual and the environment is mediated by the cognitive structures of the individual......and what we learn from the environment is dependent upon our own structuring of those experiences." (Nystedt and Magnusson 1982, p34).
The Centre for Independent Studies uses a 'Trends in Disability Support' graph from the Australian Bureau of Statistics (2002) to demonstrate that over half of the 5% of Australians that are on a disability dependency payment (p83) are claiming Musculoskeletal and Psychological disability. This highlights the need to evaluate cost-benefit ratios employing the language of politicians, bureaucrats, autocrats and their economic advisors. Therefore, people with health economic modeling capabilities are required, who can argue clinical relevance based on multi-factorial and projective variables of productivity and vitality. Unfortunately, in a power structured adversarial society, unless the Australian Physiotherapy Association employs such people, like Herr K, the profession may be condemned by uneconomic time constraints resulting in inadequate treatment outcomes. Could academics, clinicians and statisticians be hired for such a role?
Unfortunately, there is such a high burn-out rate amongst clinicians. .A balance between pragmatism and idealism must arise as a clinician strives for excellence. Ethical and moral factors may underpin some clinical and business decision making. Generally, the running of a private practice requires the administration of multiple tasks for which the clinician has neither economics nor business training. Young graduates seem surprised at the meager income of a clinician when they compare this to other professions with similar or generally much lower matriculation scores required to enter university (physiotherapy TER's have been in the 95% plus range for over a decade). It is of little surprise that they all wish to administer exercise programs, with 'hands on physiotherapy' being regarded by young physiotherapists as too wearing on their own bodies, and representing too little remuneration in a city as expensive as Sydney. Moreover, administering exercise is an easier cognitive premise than the rigorous process of clinical reasoning which deals one-on-one with a person's problems. Additionally, with academics fearing 'patient dependency', the view that exercise is preferential to 'hands on' treatment is reinforced. The reality is, that 'hands on' treatment can be viewed as 'exercise enabling' as well as providing cognitive feedback with respect to diagnosis and prognosis through assessment and re-assessment of disability and impairment. Moreover, the 'hands on' clinician has more time to evaluate allostatic loading capacity and the clients response to potential 'yellow and blue flags', which can be amenable to a cognitive behavioural therapy approach to specific goal oriented exercise as well as education. Importantly, the clinician can screen for 'red flags' which may require careful monitoring and/or surgical intervention.
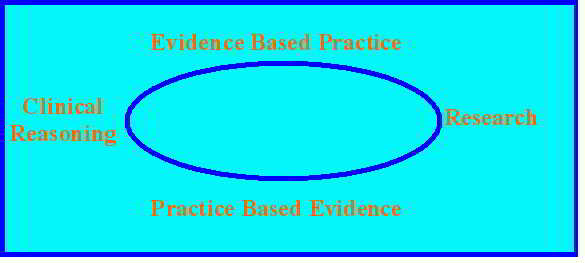
Unfortunately, the 'hands on' physiotherapist ends up a victim of their own success when they physically cannot work more than 60 hours per week trying to meet the demands of the public. With a whole generation of young Sydney University physiotherapy graduates seeming to think that 'any' exercise therapy and 'being nice to people' is the only way to tackle multi-dimensional musculoskeletal dysfunction, it is no wonder that NSW private practitioners are having severe problems with recruiting. Worse still, is the tendency for inexperienced physiotherapist to only use Evidence Based Practice without the skills nor the knowledge to undertake Practice Based Evidence. The art and craft of listening to people and defining what is important to the patient seems to have been lost amongst the hubris of apparently unsupportive scientific evidence.
More sensationalism occurred around Dr Chris Maher's work in late 2007 where mainstream national media both in Australia and the UK revelled in the apparent uselessness of physiotherapy in the treatment of acute low back pain. Who is out of touch here? If truth is a construct based on the relativity of knowledge, then could an experienced clinician be closer to the truth than certain researchers with naïve reductionist paradigms? Moreover, since the vast majority of physiotherapists in NSW, at that time, were trained at Cumberland College/Sydney University, does this mean that the School of Physiotherapy will critically appraise it's own core curriculum and teaching methodologies? Is it true to say, that the last far reaching innovative idea in Musculoskeletal Physiotherapy from Cumberland College/Sydney Uni was from Jenny McConnell and her motor control - taping techniques for the knee, in 1985? Hence, could this mean that more innovative and daring musculoskeletal research will be done by Sydney Uni's School of Physiotherapy to ascertain how to improve the efficacy of their own teaching which then dictates improved clinical practice? In this manner could it follow the Schools of Physiotherapy at Queensland University and Curtin University whereby, over the past decade, they have fundamentally changed the way we approach musculoskeletal physiotherapy? Innovative new ideas, rather than the parasitic approach of feeding off festering wounds, an unnerving symbiosis of poorly trained graduates and teachers/researchers basing their entire existence on negative research, on their own graduates, in order to justify their own existence!!!!???.
Interestingly, Chris Maher's personal communication stated that 'he was sick and tired of everyone saying that the School of Physiotherapy at Sydney University only publishes negative research'. Overall, both he and the APA were surprised at the vehemence of the memberships reaction to the media reports. How can they be so out of touch, not to realise that this is dealing with peoples existence and maybe their underlying aggression towards the people who taught them the profession is founded on the lack of prior warnings, which may have included statements such as "The fundamental principles of Musculoskeletal Physiotherapy are baseless innuendo"? Perhaps, similar to warnings about cancer on cigarette packets the School of Physiotherapy at Sydney University should clearly define the hopeless nature of musculoskeletal physiotherapy, in treating low back pain, to all intending applicants to the course? Alternatively, the aggression may be more likely to be the perception that the onus is on the clinician to change the way they do things to demonstrate efficacy in clinical practice? Perhaps the clinician needs to "ask not what your researcher can do for you, but what you can do for your researchers"? (pardon the paraphrasing). I certainly whole heartedly agree that the management of musculoskeletal conditions must include the clinical reasoning approach which incorporates continuous demonstrations of efficacy whilst using and enhancing 'evidence based practice' with 'practice based evidence'. However, do we need our own insecurities published to the world? Would they be better published to a physiotherapy audience? Would the reaction be the same? Will this create positive change or more pessimism, learned helplessness and burnout?
"The path to hell is paved with good intentions"
Make no mistake about it, Dr Chris Maher's research over that past decade had far reaching consequences for physiotherapists treating low back pain. It may well be that, in the future, insurers will refuse to pay for such treatment. It is even possible that any physiotherapist treating low back pain may be charged with over-servicing. Perhaps it is time for clinicians and academics to come together and develop more meaningful research paradigms where the process of validation is addressed by defining the essential clinical questions?
Since the early 1990's we have witnessed serious shortfalls in funding resources for health due to the demands of increasing burdens from an aging population or from the spread of serious disease (metabolic syndrome). The physiotherapy profession as a whole have been extremely pre-emptive in their quest to validate the efficacy of their health management systems. Where major changes to health systems are imposed by policy committees, which do not represent the interests of all stake holders (clinicians, patients, insurers), then disenchantment and burn-out from all disempowered clinicians and patients are likely to follow. More alarmingly, this may have severe and far reaching consequences on the quality of treatment, early access to appropriate treatment and hence the future costs of health for many Australians.
Clinical focus and to whom does the cost-benefit ratio belong?
precipitating factors -> injury -> consequences of the injury with adequate/inadequate/delayed intervention
As musculoskeletal physiotherapists we can frequently resolve the acute/sub-acute injury within 3-6 treatments using 'pattern recognition' and relatively standardized treatment approaches. However, if we use a clinical reasoning approach examining cause and effect there may be multiple structures which may need treatment. For example, with lumbar spine radiculopathy, initial treatment may involve sustained rotation and/or mechanical traction as well as some simple transverse abdominal exercises and breathing. However, examination of the mechanisms leading up to the injury may suggest reduced muscular compliance in the lower limbs, stiffness in the thoracic spine leading to reduced lateral thoracic expansion required for adequate diaphragm activation. The consequences of the injury may be muscle spasms in the multifidus, erector spinae, piriformis, hamstrings, calfs and Psoas Major accompanied by deactivation of the deep hip, pelvic, and abdominal stabilizers leading to alterations in lumbo-pelvic rhythm from reduced proprioception as well as corrupted motor control. At a standard physiotherapy consultation of $75.- per treatment, the primary symptoms can be quickly treated leading to a highly profitable practice when working at 3 patients an hour. The physiotherapist can be heartened by the fact that most of these conditions will resolve spontaneously and hence they only need to worry about not exacerbating the condition. However, as a Musculoskeletal Physiotherapist and Exercise & Sports Scientist for me to examine and respond to the multi-dimensional and multi-factorial problem (cause & effect) in a multi-modal manner, I need at least 40 minutes per treatment session. Here, I would need to assess neurological signs and symptoms, examine multiple joint structures using various techniques, examine muscles for the strength, power, endurance, flexibility, and timing of action, as well as consider motor control. Additionally, I would need to address psychosocial issues as well as general health issues resulting from a general lack of exercise. Hereby, the validity of the diagnostic procedure are enhanced whereby disability and impairment measures are used to demonstrate the efficacy of the treatment. A Clinical Psychologist can charge $180- per treatment and an Exercise Physiologist charges $150.-. Suddenly, the highly qualified and undervalued Musculoskeletal Physiotherapy clinical reasoning approach, using 'state-of-art' reasoning and treatment becomes very uneconomical at $95.- per 40 minute treatment session. Even the basically qualified masseur charges at least this if not more. Therefore, what is the incentive for Musculoskeletal Physiotherapists? Apart from the incentive of ethics and morality, the harshness of reality is that we need to feed our family after taking off 2/3 of our income to pay for the over-heads of running a business. Moreover, in a society where 'might is right' it values those principles which make people wealthy as this is regarded as synonymous with success
Recently, I had a client who sprained their ankle on some stairs at work. They worked in a high pressured environment and had young children. Their stress relief was to go running. Additionally, they had commenced running some years ago because it helped alleviate their low back pain from sitting at a desk all day. Due to the ankle sprain, they had to stop running. This resulted in less coping with stress and a gradual increase in their previous low back pain. This created some anxiety as the back pain had been severe in the past. There was also some irritability with work colleagues, wife and children because s/he wasn't getting out for their usual runs with their friends. This made them a little depressed, especially since the ankle injury was slow to resolve, and their low back pain was preventing them from lifting their 6 month old baby and playing with their 2 year old. Obviously, psycho-social factors are becoming dominant. So, what is the solution? CBT? Goal setting and reassurance? Yoga and transcendental meditation? Fixing the sprained ankle? Clearly, ankle impairment and hence disability is the causative factor which has the potential to resolve all the other factors. Yet, in non-specific low back pain is causation a measurable factor? If the client is still at work, then Workcover has achieved it's outcome goal. Since part of evidence based practice should incorporate the "values and beliefs of the client" then is this satisfactory for the client who is unable to participate in the day-to-day care of their family or in their social interaction in sport?

At the MPA conference in Sydney in 2003, Professor Richard Deyo described a professional baseball player who returned rapidly to National League baseball after an injury. By referring to the newspaper sports results, he most poignantly demonstrated that although he had made a quick return to work (RTW), his run and strike rate had dropped dramatically. No doubt the Workcover equivalent in the USA was overjoyed at the quick RTW for a professional baseball player. However, what did the club president, coach, shareholders, and advertisers think of the loss of form of their star player? Importantly, how is productivity measured? In a Psycho-social domain?
Psychometric measurements were examined in the past decade to determine what constitutes optimal treatment outcome. However, the argument is circular, since neither optimal treatments nor optimal psychometric measures have been defined. Unfortunately, lack of either has been used to emphasise the inefficacy of physiotherapy for the treatment of non specific low back pain. Clearly, these measures need to be context specific. Importantly, disability and impairment can create issues in the psycho-social domain, which in turn can create further disability and impairment.
To the constructivist, knowledge is not a precise map of external reality but a schemata or cognitive structure which can be compared or tested to other peoples construction of the same situation through the use of workable hypothesis or templates (Candy 1991, p 265). Domain specific prior knowledge plays a significant role in the process of construction, problem solving and learning. Systematic procedures for problem solving can be learnt which if content and context specific can lead to advanced clinical reasoning where errors in heuristic procedures can be detected immediately through the continuous testing of the working hypothesis and it's evaluation of the relevance of clinical data to the specific problem at hand. Hereby, not only can reliance on 'heuristics' be monitored but new schemata can be construed from the clinical environment when a clinical presentation occurs with which the clinician is unfamiliar.
It is just as important for scientists to be clinicians, as clinicians to be scientists. As the science evolves, the questions which arise shouldn't be used to denigrate but rather ameliorate clinician insecurities. Since the work is still in progress, the knowledge generated should empower the clinician to better themselves. Similarly, the specialist clinician should empower the research scientist to be able to 'ask the relevant questions'. Otherwise, research paradigms using sub-optimal treatment to determine optimal outcomes will continue to generate confusion. This confusion could potentially be manipulated to reduce clinician credibility.
"All desperation carries the seeds of it's own demise" (Petrarch)
or
"There is no virtue without terror" (Robespierre)
Buckingham, Jennifer (2004). State of the Nation : an agenda for change. The Centre for Independent Studies. www.cis.org.au
Nietzsche F. Also sprach Zarathustra. Goldmanns Gelbe Taschenbuch, Munich
Khun, TS The Structure of Scientific Revolutions
Philosophy of the Mind
An exciting approach to challenging realities is the examination of the Pain and Philosophy of the Mind (Alex Cahana July 2007, Pain Clinical Updates, Vol XV, 5). Cahana argues that 'mind-body supervenience' (physicalism or materialism) where pain always has a physical substrate, isn't enough to explain the qualitative nature/character of pain ("qualia" = what it is to be).

The problem with physicalism as argued by Cahana is that 'you are nothing but your synapses' ("eliminative") or 'you are ultimately your synapses' ("reductive" or "token").

This latter statement is reminiscent of the oration given by the late Professor Patrick Wall's at the Moving in on Pain conference in Adelaide in 1995. He was known originally for the 'pain-gate theory' which in his later years he'd redefined to cortical descending modulation of those original 'pain gates'. Since the advent of brain imaging in the 2010's these perceptions and postulations have been vindicated.
Cahana (2007) concludes by stating that "pain cannot be separated from the person experiencing it, and the human experience cannot be omitted from a scientific explanation of how our mind works. Therefore, a new subjectivist, interpretive, phenomenological stance is needed in order to capture the complexity of the patient's narrative experience (narrative dyad)".

Fear connotes an identifiable threat (eg in Australia the King Brown snake - one of the most venomous in the world), whereas anxiety connotes the possibility of threat. Fear-avoidance relates to the behaviour that an identified activity may have (real or imaginary). Kinesiophobia refers to the patient experiencing "an excessive, irrational, and debilitating fear of physical movement and activity resulting from a feeling of vulnerability to painful injury or reinjury" (Kori SH et al Pain Management 1990; Jan/Feb:35-43)
Avoidance behaviours occur in anticipation of pain and generally persist because there are few opportunities to correct the erroneous expectations which drive them. This has a deleterious effect in the engagement of ADL (activities of daily living) which then in turn can lead to mood disturbances, irritability, frustration and depression. The fear-avoidance behaviour leads to secondary consequences of deconditioning whereby normal activity such as carrying the shopping leads to excessive fatigue, heart palpitations, nausea and distress.

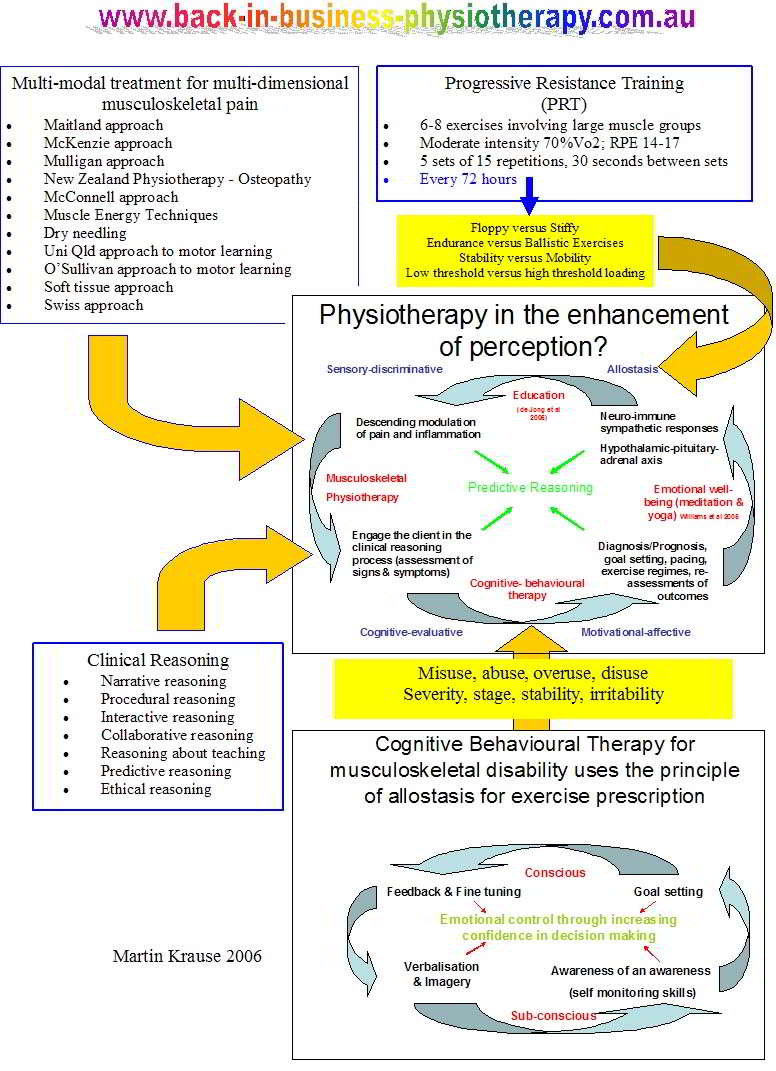
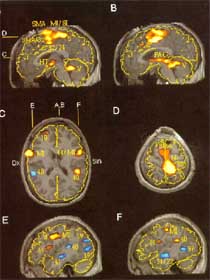
Cognitive behavioural therapy (CBT) focuses on the content of the disorder which has lead to the excessive behaviour. Through progressive cognitive appraisal and re-appraisal the irrationality of the behaviour is reduced. Another method of dealing with mal-adaptive behaviour is to recognise the behaviour for what it is and attempt to associate this behaviour with positive thoughts, experiences and activities. Hereby, neurons that fire together, wire together into a positive movement experience. The original fear & anxiety may not be extinguished but the ability 'to move on' and the ability to neither dwell on the anxiety nor on the content of that anxiety is taught and learned. Importantly, education into how the brain processes and deals with information, using PET scans, fMRI's, flow diagrams, etc become very useful tools when explaining the usefulness of graded motor imaging (GMI) tasks. Recently, however, Lorrimer Moseley has suggested to firstly use computer generated images to distinguish any signs of cortical laterality bias either towards or away from the affected region. This appears to be particularly useful for anterior knee pain, CRPS, frozen shoulder and neuropathic limb pain, but may not be so relevant to spinal pain. Never-the-less, recognition and education of the problem are paramount to successful outcome.
click on image for greater resolution
"Living in the past is dwelling upon what cannot be changed, living in the future is creating the milieu for fear and anxiety, living in the now is the right environment for action and change"

Traditionally, pain impulses were though to affect cortical activity in a fixed manner. However, cortical interaction not only is influenced by pain impulses it can change the interpretation of pain impulses, as well as change the behaviour towards those impulses. The brain is remarkarbly malleable to change, demonstrating functional plasticity to various management strategies.
Altered Cortical Processing isn't simply an amplification of subcortical input : see Tinazzi et al (2000)

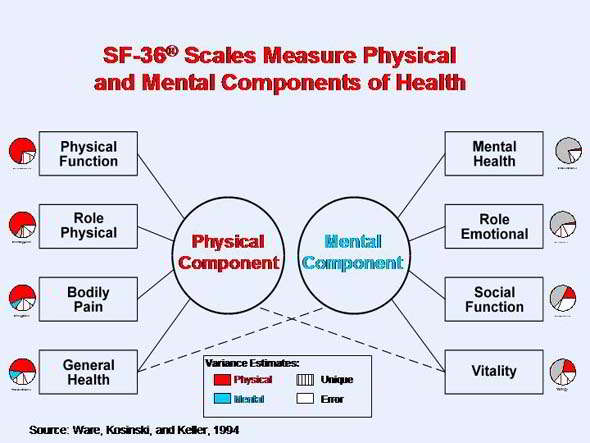
http://www.sf-36.org/tools/SF36.shtml
The Pain Anxiety Symptoms Scale (PASS) validity has been supported by positive correlations with measures of anxiety, cognitive errors, depression, and disability.
Fear of Work Related Activity = Fear - Avoidance Beliefs Questionnaire (FABQ) has 2 parts, one on physical activity, the other on work. The latter has been shown to have significant predictive validity with disability in ADL and days off work, more so than biomedical parameters such as anatomical pattern of pain, temporal pattern, and pain intensity.
Fear of movement = Tampa scale for kinesiophobia (TSK) is a 17 item scale to assess the fear of re-injury due to movement.
Reducing Pain-Related Fear
Peter Lang's bioinformational theory of fear (J Affective Disorders 2000; 61:137-159) predicts to reduce fear
- the network mediating the fear needs to be activated
- new information needs to be presented to discredit the expectations that are inherent to the fear memory.
Demystification of the pain through education, appropriate treatment with graded exposure which includes operant cognitive behavioural activity parameters are the cornerstone of such an approach. Paradoxically, verbal re-assurance may have the opposite affect and lead to increased distress.
Non specific low back pain
The 5th international congress in low back pain concluded last week in Melbourne (Nov 2004). Apart from the usual palabra, there seemed to be some common sense coming from the floor into the discussions. The great proponents of reductionist paradigms for studying so called 'non-specific low back pain' came under fire for the 10 years of misdirected and misguided research trying to identify specific variables using a non-specific paradigm. Cognitive factors, including beliefs, depression, kinesiophobia were thought to make up around 50% of measurable outcome variables, disability 30% and impairment only 20%. Whilst the statistical methodology & reasoning was highly commendable, the premise of a lot of research on the efficacy of treatment interventions was that all physiotherapists are equal. It would seem ludicrous that the same proponents of graduate programmes in Musculoskeletal and Sports Physiotherapy can rationalise that the skill level of the physiotherapist is irrelevant to outcome. These arguments seem to have arisen from poorly designed investigations in the mid 90's.

Impairment measures are traditionally seen as 'range of movement' and sometimes neurological impairment. However, more difficult measures which usually aren't included in impairment measures are quality of movement, and the muscle activation required for the distribution of force across joints and between body segments ( inverse dynamics and Newtons 3rd Law). Additionally, when considering the 'mass-spring' analogy of movement and energy conservation, then perturbations of movement and the capture of energy from perturbations of movement, such as plyometrics , become important aspects in the clinical reasoning paradigm. Yet, how are these measured in the NSLBP paradigm by traditional 'non-progressive' research.
Those same protagonists also argued in the 1990's that there was no role for dose in manual therapy. (Dose representing the force, duration, frequency, number of repetitions, the type of technique used commiserate with the stage, stability, severity and irritability of the disorder as well as based on the identification of the 'cause of the cause' of the dysfunction). Additionally, back in the 1990's they used placebo constructs which ignored the fundamental role of higher centres in pain and information processing. Even the paper which I submitted to Manual Therapy for publication on mechanical traction had the descending modulation and cortical modulation aspects deleted from it by the co-authors.
Thankfully, multi-modal treatment approaches are now receiving some credibility as a research paradigm. Additionally, the biomechanics and specific treatment intervention for pelvic girdle dysfunction is being extracted out of the NSLBP paradigm. Progressive research on impairment and specifically the importance of muscular forces are being performed by Wim Dankearts under the guidance of Peter O'Sullivan. They are working towards a novel classification system for non specific chronic low back pain patients which includes higher order mental processing. This classification system is based on behavioural influences on movement as well as the directional limitation of the dysfunctional movement. Specifically, Peter O'Sullivan has put forward 3 sub-categories
-
"Pain disorders associated with movement impairments are associated with a loss of normal physiological movement of lumbo-pelvic mobility, and abnormally high levels of muscle guarding and co-contraction of lumbo-pelvic muscles with generation of intra-abdominal pressure....[resulting in].....excessive force closure"
-
"Pain disorders associated with control impairment are associated with no impairment to the mobility of the symptomatic spinal segment, but rather present with impairments or deficits in control of the symptomatic spinal segment pressure...[resulting in]....reduced force closure"
-
"......mal-adaptive movement and motor patterns result in chronic abnormal tissue loading and ongoing pain and distress......These disorders are also invariably associated with non-organic factors but these factors do not dominate the disorder, leaving them more amenable to physiotherapy intervention based on a cognitive behavioural motor learning model"
(5th Interdisciplinary World Congress on Low Back and Pelvic Pain, Melbourne, 2004, Australia p132)

Unfortunately, the non-specific paradigm has given the ammunition needed for proponents to suggest that any exercise regime is better than something based on a clinical reasoning process administered by highly qualified physiotherapists using 'state of the art' research coming out of Europe, Queensland and Western Australia. Ironically, in the medical profession, if you specialise your remuneration increases, whereas in physiotherapy the prevailing argument (in NSW) suggests that you are wasting everybody's time and money because "85% of low back pain is non-specific". I'll let you decide the absurdity or otherwise of this paradigm.
The APA actively promotes the new title of specialization, yet this is meaningless if there is little promotion of the already existing titled members. There is also little standardization of fees charged by titled members as this would lead to charges of collusion by the ACCC. It then becomes increasingly difficult for individuals to charge the public more, if the public have no idea what value they are getting for their money. Some clinicians have commenced using item descriptors to charge their clients more when being treated by a more highly qualified physiotherapist. Ironically, I would suggest that close to 100% of the adult population knows what a chiropractor does, but that hardly anyone knows what a Musculoskeletal Physiotherapist does!!!! Even concepts evolved from research into Musculoskeletal Physiotherapy, such as 'core stability' are perceived by the public to be something which happens at the gym and hence belongs to the Exercise & Sports science profession!!!!!!!!!!!!
in the 1980's to mid 1990's, there was extreme competition to gain entry into post graduate Manipulative Physiotherapy. Once in the course, students worked 24/24 -7/7 and needed to complete research just to get through a graduate diploma, whereas the Masters required 1.5-2 years. Generally, most post graduate courses have been diluted and made easier where a double Masters degree without a research component can be gained within a year. Such dilution was due to funding as well as making the course more attractive to non-suffering types. Moreover, the introduction of entry level Masters Programmes of Physiotherapy may have further diluted the perceived value of titled post graduate Musculoskeletal qualifications. Yet, In some instances this easing of entry and completion requirements may be a reflection on the reduced clinical and theoretical competencies of both the people teaching the courses as well as those taking the courses? In fact, experienced clinicians in this State have been left wondering why graduates have such poor clinical skills. They seem to have a lot of trouble even defining 'function' let alone dysfunction. Their movements analysis skills are reduced to goniometers and tape measures, where analysis in the quality of movement seems impossible. This suggests to me that graduate entry Masters Physiotherapy courses make a lot of sense if they are preceded by a degree in Exercise and Sports Science, similar to that offered at Griffith University. However, that leaves us then with the problem of 'what next'?
Since there is little promotion of post graduate skills to the public, is it little wonder that very few Australians attend these University courses. Even worse, some Universities spent a decade denigrating the profession's treatment of low back pain in their search for the holy grail of the 'ultimate psychometric evaluation'. A recent article (Inmotion August 2006) by a highly successful private practitioner in Sydney, Jospehine Key, highlighted the poor clinical capability of many of the post graduate people she interviews. She laments the attitude of the major local institution that "if you can't prove it then you can't teach it", and furthermore she believes that the public place more faith in the "new experts" who are "the gym instructors and personal trainers, the fitness specialists, the Pilates and Yoga teachers, and even exercise physiologists". Furthermore, she makes a highly valid point by stating the undergraduate/postgraduate physiotherapists receive far less supervised contact time than those studying osteopathy or chiropractic. Hence, she concludes that the discerning consumer will choose to go elsewhere if we cannot deliver.
The reality is that post graduate courses represent an extremely expensive option of around $20,000 in student fees as well as lost income from taking a year out of work. Hence these courses are now attended by foreign students who return to their country of origin and are idolized for their knowledge. They frequently open successful practices and partake in delivering continuing education - lecture tours where a few hundred thousand dollars a year remuneration is not uncommon. The average income of Australian physiotherapists is around $60-90,000per annum, generally regardless of post graduate qualification. Interestingly, the profession seems to be coming full circle, whereby physiotherapists in some countries (e.g. Chile & Switzerland) are undertaking post graduate Osteopathy courses rather than Physiotherapy courses. This is similar to Australasian physiotherapists in the late 1960's/ early 1970's attending Osteopathy courses in the UK to gain post graduate experience. Those therapists in turn worked on creating the first post graduate physiotherapy courses in Manipulative Physiotherapy. Is this the beginning of the end? In recent years, the undergraduate physiotherapy course has become a conduit for entry into medicine. Although, the number of physiotherapists undertaking post-graduate medicine are small, their number would be in the vicinity of those who used to undertake post graduate physiotherapy courses.
A current solution seems to be clinician - university partnerships whereby private practitioners engage and pay for University amenities whilst offering private post graduate qualifications. Tobby Hall and Kim Robinson are both Mulligan Instructors who have developed a post graduate course of instruction with Curtin University. This partially solves the problem of private consortiums such as those in Europe generating decades of profits from education based on Australian Research paid by the Australian tax payer. On a brighter note, a new Masters Programme in both Sports and Musculoskeletal Physiotherapy has been developed in conjunction with Donau University Krems and PhysioAustria. This is a major new development when one considers that 20 years ago, the qualification of an Austrian Physiotherapist was "an assistant in physical and rehabilitation medicine" which involved 2 years of non-university study. Hence, is Australia still leading the world in Physiotherapy or falling behind it? What are the role of private-public partnerships in clinical education and should some of their profits be funding University based research?
The dropping numbers of students aren't confined to Physiotherapy specialised post graduate courses and has been attributed to Australian federal government policy. The Financial Review 28 August 2006 describe a massive drop by 18% in the number of all new enrolments by Australian students starting university, between 2002 and 2005. Craig Emmerson, the opposition spokesman stated on ABC's Lateline (08/09/2006) that spending on training in real terms by the Australian government has gone backwards by 8 per cent, whereas for the rest of the OECD, it's gone forward by 38 per cent over the same period. Sadly, the Australian Musculoskeletal & Sports Post Graduate Physiotherapy education program is in danger of becoming extinct due to lack of local enrolment as well as poorly federally funded clinical education components of the courses Previously, these courses relied on the altruism of physiotherapists devoting their time and knowledge for the greater good. In fact, this free website reflects the importance I place to the continuing development of the profession. Interested readers should refer to the article on the dire future of Post Graduate Physiotherapy education by Gwen Jull and Peter O'Sullivan in the June 2006 edition of the Australian Journal of Physiotherapy. The APA and profession at large must act now by promoting the superior skills of physiotherapists with post graduate qualifications, otherwise the ultimate paradigm shift will inevitably occur.
Just prior to his assassination, Martin Luther King Jr. said in a speech "We are now faced with the fact, my friends, that tomorrow is today. We are confronted with the fierce urgency of now. In this unfolding conundrum of life and history, there is such a thing as being too late. "Procrastination is still the thief of time. Life often leaves us standing bare, naked, and dejected with a lost opportunity. The tide in the affairs of men does not remain at flood - it ebbs. We may cry out desperately for time to pause in her passage, but time is adamant to every plea and rushes on. Over the bleached bones and jumbled residues of numerous civilizations are written the pathetic words 'Too late'. There is an invisible book of life that faithfully records our vigilance in our neglect. Omar Khayyam is right: 'The moving finger writes and having written moves on' ".
Advances in Extended Scope Practice for Physiotherapy career development
- the future?
The June 2005 inmotion publication of the APA noted some interesting developments in the U.K. Physiotherapists are being trained in Accident & Emergency triage procedures in addition to others being trained to perform arthroscopies by the end of the year! This up-training is apparently due to the imminent shortage of qualified medical practitioners as a result of the ever increasing age of the baby-boomer demographic. In Victoria, Australia, physiotherapists are covering musculoskeletal assessments in the Accident & Emergency department of the Royal Melbourne Hospital. These developments are particularly interesting in that they represent a new and exciting career path for physiotherapists. Lack of career path and poor recognition of skills by the public and other health professions has been suggested as a disincentive for people to remain in the profession or even to take up physiotherapy as a career in the first place. In the USA for example, it appears to be becoming ever more difficult to entice graduates into a Physical Therapy programme due to the considerable costs of education and poor prospects for remuneration once they have graduated. Similarly, in Australia, where the matriculation entry level (TER) is in the the top few % of the state, new graduates are frequently bewildered to find that their student colleagues who had much lower TER's were earning a lot more than them. Furthermore, the ceiling in earning capacity is reached very quickly leading to physiotherapists working longer hours, with no 'downtime' causing either physical injury and/or burnout in over 1/3 of graduates. The recent developments in the UK may represent a potential remedy for the chronic shortage of skilled physiotherapists by representing an exciting new career path with considerable potential for personal and professional development?
"Liberate your mind and only then will you find your freedom"
Malcom X
The case of Lance Armstrong
We are all familiar with the case of Lance Armstrong, the man who survived testicular cancer with metastases throughout his body, who returned to fight another day and win 7 Tour de France titles in the process. The effect on the general public was astounding. A million people stood on Alp D'Huez, to see the man who defied the boundaries of our imagination. He gave hope and inspiration to millions of people suffering from cancer and along the way created a charity which raised $1/2 billion over several years. At the Tour Down Under, 100,000 people lined the streets and his presence raised $1/4million in gold coin donations as well as gaining government commitment of $45million for cancer research at Adelaide Hospital.
This all came to a screaming halt in September 2012, when he refused to defend himself any further, on doping charges. Although, he had passed over 500 doping tests, and samples were stored for 8 years and re-tested, the allegations against him wouldn't go away. The bulk of the evidence against him was from disgruntled former team members who had been caught for doping with EPO. Additionally, one vile of EPO was apparently discovered by a journalist by accident, which could be traced back to Lance. He now has a life-time ban against participation in both amateur and professional sports. The first ban was the Boston Marathon which he was due to race on 7 October 2012. He said he was participating in this event to raise money for his LiveStrong Charity.
Several moral and ethical issues arise here. It would seem that during the time of his reign everyone was cheating. Hence, it could be argued he was doing what everyone else was doing, and in fact being stripped of his titles gives one of the victories of the Tour de France to Vinakurov who served a 2 year ban due to doping. In fact, some anecdotal accounts suggest that Cadel Evans 5th place in the Tour could be translated to a first if everyone who has been caught for doping since then was removed from the list!! One argument suggests that we need to consider where Lance came from. Prior to his cancer he weighed over 100kg, after his return to elite sport he was in the 70kg range, yet he still had a heart for a big engine. What the cancer allowed him to do was reform his body shape to be a mountain climbing cyclist (superb power-weight ratios). Obviously, during the cancer, Lance was probably on every known doping substance. Afterwards, he was left with no testicles but he had the balls to make a come-back in a sport which had almost forgotten him. In so doing, he changed the sport, the way teams trained and prepared, and brought millions of viewers to the sport. Unfortunately, millions of viewers become an interesting proposition to sponsors and advertisers. In sports where the stakes are high, the temptations of making money through dubious means increase. An argument exists that this doesn't just apply to the athletes, but to everyone involved with the sport. Hence a culture is nurtured with possible ethical and moral standards which are far from sanctimonious. Where is the limit of this moral abyss. It could be argued that 'everyone in the scene knew' and that this culture of 'ormeta' extended to any town, village and city which had anything to do with hosting the sport, and where money was made by attracting tourists, etc to a tainted event.
After, so many year, was there any point in pursing the doping allegations? Does this set an example to younger riders? Will Armstrongs' wealth diminish as a result of the ban? Would it have been more pragmatic to look towards the future rather than pursue the past? The future may have been a cure for cancer or at least a major break through. Has revealing the truth of the past created a better society? Only time will tell. I certainly cannot condone cheating, but I would like to think that, similar to 'crime and punishment', after committing the crime the catharsis is emblematic of what the protagonist does afterwards to atone for their sins and create a better world. So if everyone 'comes clean' will it be possible to start afresh, with a new generation of organisers and athletes, or will a culture of greed and corruption continue? Will it stop at cycling, or will other sporting bodies investigate known associations of athletes and management with likes of Michel Ferrarri? At the end of the day, will we be richer for the experience or poorer and more cynical?
Finally, in early 2013, Armstrong confessed to cheating, using EPO, steroids and blood transfusions. In the interview with Oprah Winfry he demonstrated little remorse, except when he mentioned his guilt when talking to his son. It now transpires that he sued several people over his doping accusations. Apparently, his personal wealth of $150,000,000 is now in jeopardy and that he wishes to continue to compete in triathlons. What hasn't transpired, are the people and organisations which helped formulate the 'most comprehensive doping regime ever scene in modern sport'. The facts are that others had been driven to suicide over doping scandals and allegations. Furthermore, it would appear, Michelle Ferrari has had links with other sports such as soccer and tennis. Having spent several years working with elite and professional athletes, I have personally seen the corruption which are accompanied the machinations of 'big business' and 'national interests'. How people within sporting bodies are transformed when the sport becomes an Olympic event and everyone wants a slice of the action. However, do we want to know these 'truths' when ignorance is bliss. It must be remembered that the passion of fans to identify in some 'primitive and tribal' manner towards their sporting heroes plays an important role in society. Will the future hold a more morally and ethically accountable sporting agenda, or true to a Machiavellian philosophy, the means are justified by the ends?
Early 2013, the sporting world in Australia were rocked by widespread doping allegations. Several AFL and NRL teams had undergone organised doping with 'peptides' as well as evidence of 'match fixing'. Organised crime and sports betting were thought to be involved with the later. A new generation of peptides, some of which hadn't been tested on humans were thought to have been given to young professional athletes. These peptides (growth hormone releasing hexapeptide (GHRP-2 and -6), being a short chain amino acid were used to stimulate muscle growth and repair. Other substances included Australian-owned growth hormone variant AOD-9604. This protein-based hormone helps burn fat and stimulates weight loss, though does not necessarily enhance muscle strength. Presumably it would help stabilise blood glucose in endurance events, as fat would become available as an almost limitless source of energy for metabolism. Clinical trials have suggested it also helps repair muscle and tissue after strenuous activity. AOD-9604, used as a cream or injected in liquid form, is not prohibited by WADA but is also not approved for human use. Selective adrenergic receptor modulators (SARM's) have also been used by athletes since 2008. These substances work to stimulate testosterone uptake and have been banned by WADA. Insulin like growth factor (IGF-1) has also been used to promote musculoskeletal repair. It is a substance which is abundant as a child but steadily drops-off as we age. IGF-1, which is injected in liquid form, is on WADA's prohibited list. Mechano growth factor, which is injected in liquid form, is a variant of the IGF-1 hormone. It is released naturally in response to muscle stretching and exercise, particularly weight training. It stimulates stem cells to become part of the muscle tissue, and thus can produce fast increases in muscle mass and strength. Mechano growth factor is on WADA's prohibited list, and it is illegal to possess the hormone without a prescription.
The Australian Crime Commission report also identifies the use of a variety of substances that are not approved for human use. While not prohibited by WADA, their use is considered experimental and "off-label" because there is a lack of long-term clinical studies on the long-term impact of their use.
The substances include:
- Cerebrolysin: a peptide extract from pig brain which is used to treat Alzheimer's and stroke victims. It is said to improve cognitive and behavioural performance by enhancing the function of neurons.
- Actovegin: A filtered extract from amino-rich calf blood which leads to improved absorption of glucose and oxygen in tissue. It may enhance physical performance and stamina.
- AOD-9604: An anti-obesity drug which mimics the effects of exercise and is currently going through human clinical trials. The Australian-developed drug is designed to replicate the human growth hormone that controls the rate of fat metabolism.
- TA-65: A drug which acts on a section of the DNA and reportedly reduces ageing at the cellular level. It is said to work by targeting telomeres, which are sequences that protect the ends of chromosomes during DNA replication. Telomeres become shorter every time a cell divides, and TA-65 reportedly helps lengthen them, possibly slowing ageing.
- In terms of safety, one really has to question the vailidity of using any form of performance enhancement. These drugs are designed to over-stimulate of inhibit finally balanced homeostatic pathways in the body. If we take a historical perspective, we saw that people taking steroids ended up almost with gender change issues - men developing breast, women devoloping masculine-like features. In the case of EPO, we had young people suddenly die in their sleep or at the breakfast table. What are the side-effects going to be of these new drugs?
The ACC report was released (early 2013) only weeks after Europol announced widespread match fixing in soccer. The fact that it takes national and international law enforcement agencies highlights the ethical and moral dangers that an individual whistle blower faces when facing a culture of collusion. I had two experiences where it was illustrated to me what can happen to people when they fail. Back in the early 1990's I was involved in treating a soccer player who had the highest European transfer fee ever. The problem was, that when he went for his pre-contract medical, the medico did not find a problem with the players knee. Unfortunately for him and the player, it became a serious problem, requiring surgery and extensive rehabilitation. During this process, the medico was involved in car accident where he was killed. In another incident, during an Olympic Games a medical friend of mine attempted to instigate an investigation into suspicious injecting procedures by an athlete. He was asked to attend a meeting outside of the Olympic precinct, where he was told that his bags were being packed and that he was being put on a flight back home within a few hours. On arriving home, he was met by psychiatrists and temporarily committed to a mental institution. He has never been the same since. His career and marriage were later in ruins. In neither incident has there been any substantiated evidence of foul play. Importantly, is this why Lance Armstrong comes 'clean' on doping but not on 'how' it was possible to conduct the biggest fraud in sport of all time?
What is obvious in the culture of elite and professional sport is the feeling of 'disconnect' between them and the rest. They feel that non-athletes can go to a doctor and have medical conditions treated with appropriate medication whereas they cannot. They feel that events such as the Tour de France have become a gladiatorial spectacle, where the organisers make the courses so long and tough that there is no 'natural way' of finishing the event and making it exciting, all at the same time. And why does it have to be exciting?.......because advertisers want it so....and hence we come back to the culture of capitalism and consumerism. A simple yet highly flawed raison d'etre.
After, over a decade working with elite and professional athletes I hadn't realised how 'numb' I had become to the machinations of elite sport until one night, where I had been to a party, in Brussels, with my new girlfriend and now wife, that, as we were leaving, she stated how surprised she was how the medical professionals, present at the party, were so open about how they, as amateur athletes, had personally used various forms of blood doping, including EPO. At the time I thought 'so what'....................................each to their own......???? My indifference had made me as complicit as all the rest.
Agent of change
- Sympathetic ganglion and Whiplash Associated Disorder 1992
- International teaching 1990 - 2003 : Instructional Design
- Mechanical Traction - Neurophysiological approach 1995
- Third website on physiotherapy in the world (www.acay.com.au/~mkrause)1998
- Muscle Mass - an immune organ 2002
- Whole Body Vibration - book 2010
- Deterministic Chaos and Musculoskeletal Physiotherapy 2020
Last update : 10 October 2013
Reviewed with minor additions : 19 January 2020
 What We do
What We do What We Treat
What We Treat



















































































































