



Referred Neck Pain and Headaches, Balance, Visual Disturbance and Dizziness
Here in North Sydney we treat people daily with a wide spectrum of headaches ranging from less severe tension headaches to severe debilitating migraines, vertigo and nausea. Our treatments are directed at the cervical and thoracic spines and their accompaning muscles and fascia. Frequently, we also investigated the pelvis and low back as these can have a major influence on posture.
Some people come to us suffering from dizziness and balance disturbances not associated with BPPV. At least 3 systems contribute to our sense of balance; these include the upper cervical spine of the neck, the ears and eyes. As such, each system can compensate for some of the deficits in the other systems (also known redundancy). However, generally, the brain interprates information from these 3 systems using transcerebral and cerebellar correlations. When for example, neck pathology presents itself, it may result in excessive nociceptive (pain) input and/or reduced proprioceptive (sense of position) input. In these cases we use conventional treatments to the neck to reduce muscle spams and pain, combined with avant-guard techniques using laser pointers on the head, blindfolds and relocation exercises, occulo-motor tracking and stability tasks, as well as virtual reality training with the WiiFit to attain optimal outcomes for brain correlation.
Please read on for more information on
- Headache
- Vertigo
- Whiplash
- neurological causes (eg Migraine)
- malignancies
- problems with blood flow
- stress and tension
- biomechanical problems (dysfunctions) of the cervical and thoracic spine
Cervicogenic headache may occur due to dysfunction at the C1/2/3 levels. Such dysfunction may refer pain directly to the scalp and eyes via the greater and lesser occipital nerves.
Cervicogenic headache may also occur due to muscle spasms, reduced vertebral artery blood flow from as low as the first rib, adverse neural tension from 0/C1, C5/6, T6
Alternatively, cervicogenic headache may occur due to excessive nociceptive and mechanoceptive bombardment of the neurones in the spinal cord (WDR = wide dynamic range neurones, NS = nociceptive specific neurones). Overflow from the WDR and NS neurones into the Trigeminal nerve (Cranial nerve V) can exacerbate the frequency and duration of migraines. (See below)
peripheral sympathetic nervous system and WDR hypersensitivity
link to neurophysiology and PET scan of cortex
Link to Upper Cervical Spine Instability
Dizziness and Vertigo may also accompany headaches. These may be due to
- Benign Paroxismal Positional Vertigo which underlies a problem with the crystals in the inner ear
- Vertebral Artery compromise
- Sympathetic Nervous System dysfunction
- A mismatch between vestibular, occular and proprioceptive input

Pathology includes
- upper trapezius myalgia with increased [glutamate], [serotonin] and [interleukin] concentrations (Falla 2008)
- disturbed oxidative metabolism "moth eaten" fibres
- impaired intramuscular circulation
- increased proportion of type IIc fibres (i.e. reduced endurance fibres)
- increased fatigue
- decreased conduction velocity
- connective tissue infiltration
- activation of A-delta and C-fibres
- physical deconditioning leading to early fatigue resulting in impaired sensorimotor control (Karlberg et 1991)
- reduced acuity of muscle spindle proprioceptive input. Deep muscles of the cervical spine have a very high density of muscle spindles (Bakker & Richmond 1982)
- muscle fatigue reducing the quality of proprioceptive information (Pederson et al 1998, Johansson et al 1995)
- impaired function of the deep cervical muscles (Jull 2000)
- impaired proprioceptive input from deep cervical muscles
- impaired ability of the CNS to utilize cervical proprioceptive input
- proprioception (Jull et al 2007b)
- active repositioning tests to assess muscle and joint proprioception (efferent-afferent mismatch) (Lee et al 2006)
- passive repositioning using blindfolds (joint proprioception) - discrimination threshold and constant error
- smooth pursuit eye tracking (Treleaven et al 2005a)
- deep neck flexor muscle strength and endurance
- trapezius and levator scapulae muscle activity
- passive joint moblizations
- passive and active ROM
- postural sway (Treleaven et al 2005b)
- shoulder strength and endurance
- shoulder acuity and repositioning with cognitive-behavioural aspects of kinesiophobia (Djupsjoebacka 2008)
- psychometric evaluation (Neck Disability Index)
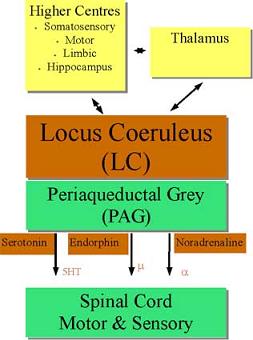
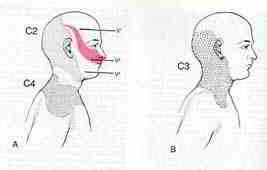 Cervical Headache : the relationship of upper cervical spine (O-C3) dysfunction and the trigeminal nerve. The International Headache Society (IHS) classification of headache is based on clinical phenomenology which assumes that a common presentation defines a valid pathological entity. Migraine and cervicogenic headaches (CH) have a number of common features which need to be appreciated when discussing the role of Spinal Manipulative Therapy (SMT) in migraine headache management. The structures supplied by the sensory division of the first 3 cervical nerves include " the joints and ligaments of the upper 3 cervical segments, their posterior and anterior muscles, the sternocleidomastoid and trapezius muscles, and the dura mater of the posterior cranial fossa" (Bogduk 1983). Relays in the trigeminal nucleus have been implicated in referred headache from these structures (Bogduk 1992). Physical irritation of both the greater occipital nerve (GON) and the C2 and C3 roots may cause hemicranial symptoms (Pfaffenrath, Dandekar, Pollman 1987) similar to migraine (Anthony 1989). The cell bodies in the trigeminal ganglion innervate the large cerebral arteries and dura mater (Liu-Chen, Mayberg, Moskowitz 1983). Periodic failure of the locus coereleus and raphe nuclei to suppress activity in the C2-C3 segments in the trigeminal nucleus of the spinal cord is postulated to cause migraine (Goadsby 1993). Unfortunately, the quality of CH vary greatly and don't adequately distinguish them from migraine. CH tend to increase in frequency and are more easily provoked as the lesion progresses (Edeling 1982). However, migraine rarely expresses itself more than 10 headache days per month (Olesen 1993). Unlike CH, the distribution of symptoms in migraine are usually (75%) unilateral with side shifts (Sjaastad, Stovner 1993). Prior to 1986 a number of patients fulfilling the IHS criteria of CH also fulfilled the criteria of migraine (Sjaastad, Stovner 1993). This questions whether Maitland (1986, p330), Parker, Pryor, Tupling (1980), Parker,Tupling, Pryor (1978), and Kelly (1978) were using SMT for the treatment of migraine or CH. Vernon, Steinman, Hagino (1992) describe cervicogenic dysfunction, including hypomobility in the upper cervical spine in patients with "migraine". However studies suggest different pathogenic mechanisms between CH and migraine (Bovim, Sand 1992). Differential diagnostic problems arise when they coexist (Olesen 1993). Gawel and Rothbart (1992) hypothesise that plasticity in the sensory pathways allows leakage of pain-generating activity in ever increasing numbers of neural networks until a point is reached where the cervicotrigeminal relay is involved. Cervical spine dysfunction does not in itself cause migraine but may contribute to its expression (Kidd, Nelson 1993). Conceptually, SMT treatment of inputs into these networks may disrupt this overactivity (see Zusman 1992, 1994 for review). Clinically, manipulative physiotherapists believe that overcoming movement abnormality relieves associated symptoms (Kelly 1983). Clearly, the exact sources of pathology need to be established. Jull, Bogduk, and Marsland (1988) consider SMT accurate in the diagnosis of cervical zygapophysial joint disorders. Thorough physical and subjective examination (Maitland 1986) and the use of a pain behaviour diary may implicate the 'nature and stage' of each headache disorder. Until further research is carried out, the history (Bogduk, Corrigan, Kelly, Schneider, Farr 1985), and knowledge of IHS criteria in the classification of headaches, are crucial in deciding which patients presenting with "migraine" are appropriate for SMT. Ultimately, SMT management should assist medical practitioners in establishing a possible cervical component in a "migraine" sufferer who is unresponsive to pharmacological intervention. More recent evidence suggests a major role for the re-establishment of proprioception in chronic neck and shoulder pain. Elements of motor learning and cognitive behavioural therapy should be included in treatment regimes. Interventions which enhance proprioceptive acuity include
Cervical Headache : the relationship of upper cervical spine (O-C3) dysfunction and the trigeminal nerve. The International Headache Society (IHS) classification of headache is based on clinical phenomenology which assumes that a common presentation defines a valid pathological entity. Migraine and cervicogenic headaches (CH) have a number of common features which need to be appreciated when discussing the role of Spinal Manipulative Therapy (SMT) in migraine headache management. The structures supplied by the sensory division of the first 3 cervical nerves include " the joints and ligaments of the upper 3 cervical segments, their posterior and anterior muscles, the sternocleidomastoid and trapezius muscles, and the dura mater of the posterior cranial fossa" (Bogduk 1983). Relays in the trigeminal nucleus have been implicated in referred headache from these structures (Bogduk 1992). Physical irritation of both the greater occipital nerve (GON) and the C2 and C3 roots may cause hemicranial symptoms (Pfaffenrath, Dandekar, Pollman 1987) similar to migraine (Anthony 1989). The cell bodies in the trigeminal ganglion innervate the large cerebral arteries and dura mater (Liu-Chen, Mayberg, Moskowitz 1983). Periodic failure of the locus coereleus and raphe nuclei to suppress activity in the C2-C3 segments in the trigeminal nucleus of the spinal cord is postulated to cause migraine (Goadsby 1993). Unfortunately, the quality of CH vary greatly and don't adequately distinguish them from migraine. CH tend to increase in frequency and are more easily provoked as the lesion progresses (Edeling 1982). However, migraine rarely expresses itself more than 10 headache days per month (Olesen 1993). Unlike CH, the distribution of symptoms in migraine are usually (75%) unilateral with side shifts (Sjaastad, Stovner 1993). Prior to 1986 a number of patients fulfilling the IHS criteria of CH also fulfilled the criteria of migraine (Sjaastad, Stovner 1993). This questions whether Maitland (1986, p330), Parker, Pryor, Tupling (1980), Parker,Tupling, Pryor (1978), and Kelly (1978) were using SMT for the treatment of migraine or CH. Vernon, Steinman, Hagino (1992) describe cervicogenic dysfunction, including hypomobility in the upper cervical spine in patients with "migraine". However studies suggest different pathogenic mechanisms between CH and migraine (Bovim, Sand 1992). Differential diagnostic problems arise when they coexist (Olesen 1993). Gawel and Rothbart (1992) hypothesise that plasticity in the sensory pathways allows leakage of pain-generating activity in ever increasing numbers of neural networks until a point is reached where the cervicotrigeminal relay is involved. Cervical spine dysfunction does not in itself cause migraine but may contribute to its expression (Kidd, Nelson 1993). Conceptually, SMT treatment of inputs into these networks may disrupt this overactivity (see Zusman 1992, 1994 for review). Clinically, manipulative physiotherapists believe that overcoming movement abnormality relieves associated symptoms (Kelly 1983). Clearly, the exact sources of pathology need to be established. Jull, Bogduk, and Marsland (1988) consider SMT accurate in the diagnosis of cervical zygapophysial joint disorders. Thorough physical and subjective examination (Maitland 1986) and the use of a pain behaviour diary may implicate the 'nature and stage' of each headache disorder. Until further research is carried out, the history (Bogduk, Corrigan, Kelly, Schneider, Farr 1985), and knowledge of IHS criteria in the classification of headaches, are crucial in deciding which patients presenting with "migraine" are appropriate for SMT. Ultimately, SMT management should assist medical practitioners in establishing a possible cervical component in a "migraine" sufferer who is unresponsive to pharmacological intervention. More recent evidence suggests a major role for the re-establishment of proprioception in chronic neck and shoulder pain. Elements of motor learning and cognitive behavioural therapy should be included in treatment regimes. Interventions which enhance proprioceptive acuity include
- body awareness training (Kadi et al 2000) eg Tai Chi, Alexander Technique, Dance therapy, etc
- exercises involving coordinated rapid eye, head, neck and arm movements (Fitz-Ritson 1995)
- Feldenkrais therapy (Lundblad et al 1999)
- multimodal treatment involving exercises to improve balance, neck co-ordination, and occulomotor control (Taimela et al 2000)
- proprioception to improve eye & head movement (Jull et al 2007) - occulomotor reflexes
- low intensity endurance exercise regime for the deep craniocervical flexors for postural pertubation (Falla et al 2007, Jull et al 2007)
- high intensity exercise to challenge the neck flexors is requird to reduce the fatiguability of the sternocleidomastoid and anterior scalene muscles and improve the strength of the cervical muscles (Falla et al 2007)
- joint mobilizations, taping, trigger point therapy & dry needling, soft tissue massage, EMG biofeedback training in combination with the above.

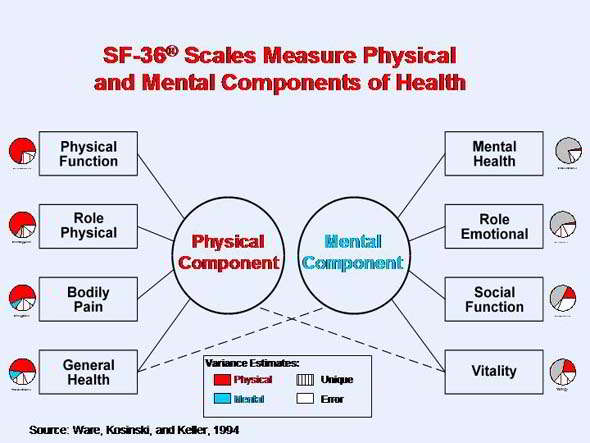
http://www.sf-36.org/tools/SF36.shtml
Cervical Proprioception
-
Clinical aspects of proprioceptive dysfunction have not been researched extensively (Kristjansson 2005)
-
Proprioception is a complex neurophysiological pathway which plays a small but important role in motor control (Gandevia & Burke 1992)
-
The cervical spine has great mobility at the expense of mechanical stability and a close neurophysiological connection to the vestibular and occular systems (Gimse et al 1996)
-
Perception drives the motor responses. Motor strategies and 'feed forward' preparatory responses are instigated by the CNS to drive the PNS. The CNS stores sensory perceptions in memory. However, sensory conflict may arise when incoming disturbed proprioceptive information is unexpected leading to altered 'efference-afference copy'
-
This hierarchical model has been criticised as it does not explain reactions to novel tasks, nor can the memory bank store all the information needed for complex co-ordinated motor tasks required to solve for the control of multiple 'degrees of freedom' problem proposed by Bernstein (1967)
-
Treatments built into hierarchical ways of thinking (Knott & Voss 1968) have been criticised for being too passive because therapeutic interventions were modelled on facilitation and inhibition rather than function training (Shumway-Cook & Woollacott 2001)
-
Systems theories examine the functioning of the whole, where self organisation occurs based on principles of physics whereby constraints within an organism, a task and the environment determine which movement strategies are best for each individual as a whole (Shumway-Cook & Woollacott 2001) - integration of neuro-musculo-skeletal with vestibular, occular and immune.
-
Clinically, treatment needs to be functionally meaningful and task dependent to appeal to the clients perceptions and cognitions.
Phylogenetics
- When the vertebrates evolved in the ocean, the whole body, including the head, formed a spindle-like unity to enable fast swimming. Spatial orientation was served by peripheral vestibular and visual systems
- About 350million years ago when vertebrates climbed onto the land, to be able to survive, their head had to be able to move freely on the rest of their body
- The first rudimentary head on neck motion was a nodding action occurring at 0/C1
- However, this wasn't enough and development of the dens axis enveloped by the ring of the atlas followed (Wolff 1998)
- Last major development took place at C2/3 which facilitated coupling of movements
- These bony developments were accompanied by distinct development of the musculature of the upper cervical spine to orient the head sensors in space
- A network of mechanoreceptors were developed to provide information of the head in regard to the rest of the body
The Cervical Spine and the Postural Control System
- the vestibular, visual and somatosensory systems
- The semicircular canals used to determine changes in the rate of motion, angular velocity
- The otoliths containing the utricular and saccular maculae provide information on linear velocity and gravity (head tilt)
- Convergence occurs in the vestibular nuclear complex (VNC) via the vestibular nerve and cerebellum
- The vestibulo- and reticular-spinal tracts provide impulse propagation to the trunk & limbs
- The upper cervical mechanoreceptors have indirect inputs into these descending tracts
Visual System & Audition
- Over 1/3 of the brain in primates is devoted to vision (Stein & Glickstein 1992)
- The visual postural system consists of 2 movement - smooth pursuit, saccade, opticokinetic
- The vestibular-ocular reflex (VOR) stabilizes images on the retina
- The position and movement of the head in relation to the rest of the body and eye movements is regulated by the VOR and the much weaker cervico-ocular reflex (COR) where the latter acts on the extra-ocular muscles.
- However, in dysfunctional conditions the COR becomes more active and can be used for differential diagnosis of upper cervical spine proprioception (Neuhuber 1998, Tjell 1998)
The somatosensory subsystem
- Upper cervical spine has an abundance of mechanoreceptors, esp. from the gamma muscle spindles (nuclear bag and nuclear chain fibres) of the deep segmental muscles (Richmond & Bakker 1982), these impulses converge in the central cervical nucleus (CNN)
- The cervical mechanoreceptors have direct inputs to the VNC via the DRG at the C2 and C3 levels which contrasts to inputs from lower spine segments which tapper off to indirect inputs.
- Inputs from lower spinal segments converge onto the cuneatus nuclei and travel from there to the cerebelllum (Neuhuber 1998)
- The CNN has important connections to the VNC. The lateral VNC is the origin of the powerful lateral vestibulospinal tracts which controls muscle tone in the trunk and extremeties (Tjell 1998)
- The cervico-collic reflex (CCR) is mediated through these pathways and probably the medial vestibolospinal tract via the VNC (Peterson et al 1985). The CCR is stimulated by cervical movements and dampens the activity of the VOR and VCR stimulated by the semi-circular canals
The nociceptive system
- The nociceptive system in the upper cervical spine projects onto many cranial afferents of which the trigeminal nucleus and the tractus solitaritus nuclear complex (Vagal nerve) are the most important ones.
- Neuroanatomical research indicates connections from the upper cervical spine to the limbic system (Feil & Herbert 1995; Neuhuber 1998)
- Coordination of movement is mainly the function of the cerebellum, where all spinal and brain stem reflexes directly or indirectly converge (Stein & Glickstein 1992)
- Linear Vestibulocollic Reflex (VCR)
- Little is known about the otoliths
- The otoliths are stimulated by linear accelerations of the head and their inputs have been found to modify both eye and head stabilizing responses (Schor et al 1985)
- Otolith contributions to compensatory eye and neck responses increased with stimulus frequency, but the otolith system alone is unable to produce perfect compensation (Boral & Lacour 1982)
- ? Convergence of canal and otolith input on vestibulospinal neurons combine to provide reflexes to linear and angular acceleration ? (Uchino et al 2000)
- ? Otoliths may have a distinct functional affect during locomotion providing compensatory head pitch movements by the angular VCR during walking and the linear VCR during running ? (Hirasaki et al 1999)
Multimodal Control
- The reflexes appear to be predominant in the frequency of natural locomotion (1.5-2Hz) (Hirasaki et al 1999) and their function is to damp oscillations of the head at higher frequencies (Keshner et al 1999)
- Voluntary responses are observed as anticipatory torques in the neck muscles or responses controlled by the occulomotor reflex
- Above 1Hz mechanical factors (inertial, stiffness and viscoelasticity) become important
- The relative importance of the VCR and CCR for head-neck stabilization is probably dependent upon the degrees of freedom and the postural requirements of the task (Keshner 2005)
Motor Control
- Complex biomechanical linkage with 20 pairs of muscles capable of performing similar actions -> therefore suggesting some redundancy in the system
- Overall the number of independently controlled muscle elements exceeds the number of degrees of freedom of neck motion -> the extent of functional variability depends upon the task being studied
- Head represents 7% body weight, yet has 20 different muscles directly linking the skull in either side of midline to the vertebral column
- Motions of the head are primarily directed towards orienting and stabilizing the position of the eyes and head in space
- CNS programmes neck muscles in specific directions rather than an infinite variety of muscle patterns
- Muscles organised in layers - outer layer connects skull with the shoulder girdle - deeper layer links the skull with the vertebra
- deepest layer consists of muscles that link the cervical and thoracic vertebrae - The layer of muscles linking the skull to the vertebrae form the long dorsal (splenius capitis, semispinalis capitus and longissimus capitis) and a long ventral (longus capitus) muscle. - > act as a sleeve for the cervical vertebrae eg rotation
- Splenius cervicis, Semispinalis cervicis, longissimus cervicis & longus colli lie deeper, have a small moment arm - > proprioceptive function
- Suboccipital muscles produce extension at the atlanto-occipital joint.
Neck muscle morphometry
- Each muscle differs in it's relative content of fast and slow twitch fibres, angles of pennation, sarcomere length, sites of origin and insertion and the mechanics of action across the individual joints
- Unlike limb muscles where there is a distinct tendonous attachment to bones, many neck muscles had very little tendons at their ends.
- Instead of distinct tendons, many neck muscles have a complex architecture of internal tendons and aponeuroses. (Kamibayashi & Richmond 1998)
Functional Synergies
- One solution to controlling the degrees of freedom (Bernstein 1967) is to organise movement around synergistic muscle torques (Buchanan et al 1989)
- In cats, dissociation between deep and superficial neck muscle activation suggests different neural controllers (Richmond et al 1992)
- Separation of two groups of muscles, one producing the forces necessary to move the head and another to align the head with the terminal target would assist the head-neck controller in meeting multiple criteria or goals (Thomson et al 1994)
- A single action can be accomplished through the activation of agonists and antagonists where the control parameter appears to be the required force vector rather than the specific force lever arm of any particular muscle (Macpherson 1988, 1991) - therefore the specific direction of motion is important
Directional tuning of muscles
- Each muscles preferred direction is unique and consistent amongst subjects (flexion for sternocleidomastoid, ipsilateral flexion for splenius capitis and extension for semispinalis capitis. Trapezius was tuned toward lateral flexion but had the lowest activation and the greatest variability)
- Rotation shifted the maximal activation vectors away from the moment arm direction due to the observation that none of these muscles produce a unique axial rotation torque (Keshner 2005)
- A likely control parameter for the CNS to employ in the selection of which muscle to employ may be contingent upon it's ability to generate a maximal mechanical advantage (Keshner et al 1997)
- Posture affecting the plane of motion of the muscles length and pulling direction may have a greater influence on its contribution than mechanical efficiency (Runciman & Richmond 1997)
- Orientation of the C/S (ie perpendicular or horizontal to earth) was a significant variable in determining the ROM, amplitude and timing of the neck muscles (Statler & Keshner 2003)
Neural Control of the Cervical Spine
- Vestibulocollic (VCR) and cervicocollic (CCR) reflexes, respond reactively to accelerotory and proprioceptive stimuli to maintain the orientation of the head in space (VCR) and the head on trunk (CCR).
- Voluntary responses are those for tracking and acquiring exteroceptive (visual, auditory and olfactory) information and can be used either anticipatorily or pursuit actions
- The normal repertoire of movement responses emerges from combinations of input and output signals (Keshner 2005)
- Vestibulospinal pathways have monosynaptic and disynaptic connections with cervical motor neurons
- Cervical proprioceptive inputs have significant influence on the vestibulospinal signals (Gdowski & McCrea 2000) and together with the reticulospinal neurones have a major influence on orientation and posture through convergence of afferent input which initiates a series of interspinal reflexes
- The VCR alone is not sufficient for purposeful head stabilization in a dynamic environment (Keshner 2005) suggesting that other inputs such as the reticulospinal are also involved.
- Gdwoski & McCrea suggest correct alignment of the head and trunk requires ascending somatosensory inputs. The CCR arises from a stretch of the neck musculature as would occur when turning the body with a fixed head position. This reflex is more complex than a monosynaptic reflex, with evidence of presynaptic inhibition in the CCR response (Banovetz et al 1995)
Neck muscle activation patterns
- Each head motion is executed by a specific muscular pattern that is not repeated in any other direction
- Motor solutions to voluntary head tracking need constant adjustment whereas the VCR and CCR probably only need to stabilize specific cervical joints.
Cervical Vertigo
- Dizziness is the third most common reason to seek medical advice in the USA (Kroenke & Mangelsdorff 1989)
1.8% in young adults to 30% in elderly (Sloane et al 2001) - Up to 80-90% of patients suffering chronic whiplash report vertigo & dizziness (Oosterveld et al 1991)
4 categories of cervical vertigo
- Vertigo : "sensation of irregular or whirling motions, either of oneself or of external objects"
- Near-syncope
- Disequilibrium
-Light headedness (40-50% of attacks are vertigo)
Differential Diagnosis with
- Vertigo (canalolithiasis and cupulolithiasis)
-Prolonged spontaneous - positional vertigo (BBPV) -recurrent attacks - Meniere's Disease
- Vestibular Neuritis
- Labyrinthitis
- Periplymphatic Fistula
- Bilateral Vestibular Dysfunction
- Central causes
- Vestibular Schwannoma
- Arnold-Chiari Malformation
- Vertiginous Migraine
- Psychogenic Dizziness
- Mal de debarquement syndrome
- Pharmacological
Cervical Vertigo
-
'spinning of the head' rather than spinning of the patient, light headedness, tipsy feeling, as a consequence of 'noise ' in the PNS
-
Usually worse in the morning and tappers during the day
-
Associated with neck movements but also with tracking an object or driving a car (Hulse & Holzl 2000)
-
Tend to increase in intensity over time as mechanoreceptors are non-adaptive and their threshold decreases over time if left untreated (Neuhuber 1998)
-
Some people don't perceive dizziness however they have overall increased muscle tone which may explain why some people go on to develop fibromyalgia
-
In long-standing cases the plasticity of the CNS (Sessle 2000) may make them treatment resistant to traditional manual therapy and techniques employing virtual reality training become important (WiiFit balance exercises), yoga, Tai Chi, etc
-
Visual disturbances although common are not widely accepted due to the lack of verification using conventional opthalmologic instruments (Hulse 1998) – these people complain of blurred vision, reduced visual field, grey spots appearing in the visual fields, temporary blindness, disordered fusion, whole words or whole sentences 'jump', double vision but not true diplopia (as with VBI), and reading problems (Hulse 1998)
-
Existence of cervical vertigo is controversial as otoneurological examination are frequently normal
-
Incidence appears to be highest in the 30-50 year old and more common in females
-
The diagnosis of cervicogenic dizziness is based on history, examination, and vestibular function tests
-
Vascular hypothesis - Vertebral artery vasospasms due to close relationship with the sympathetic nerve trunk
However this would be accompanied by serious neurological symptoms such as diplopia, dysarthria, ataxia & motor symptoms
The vertebral artery is at risk in artherosclerosis.-
Degenerative changes in the uncinate processes of the low C/S projecting osteophytes laterally, and/or subluxating superior articular processes (Bogduk 1986)
-
Full rotation of the C1/2
-
Deep fascial bands of cervical muscles crossing the artery, anomalous course of the artery between fascicles of either longus colli or scalenus anterior (Bogduk 1986)
-
-
Neurovascular hypothesis
-
Sympathetic Nervous System
-
C3/4 osteophytes and irritation of superior cervical ganglion ((Tamura 1989)
-
Direct irritation of sympathetic ganglia within fascia of anterior cervical muscles after whiplash
-
Erroneous proprioceptive signalling due to gamma reflexogenic activation of muscle spindles (Johansson & Sojka 1991)
-
However SNS blocks induces vertigo, tendency to fall, horizontal nystagmus & tinnitus, instead of diminishing the symptoms (Barre 1926, Lieou 1928 in Heikkila 2005)
-
-
Somatosensory hypothesis :
-
Disturbed afference – efference copy due to
-
Abnormal sensory input from neck proprioceptors
-
Vestibulo-occular reflex (VOR) stabilizing the visual field
-
Vestibulocollic reflex (VCR) stabilizing the head position
-
Cervicooccular (COR) proprioceptive reflex - helper reflex if the labyrinths have been damaged (Botros 1979), co-operates with the VOR for clear vision – originates in neck and joint proprioceptors
-
Cervicocollic (CCR) proprioceptive reflex – stabilizes the neck and protects from over-rotation and coutneracts the COR, probably generated by the gamma muscle spindles of the deep neck muscles (Hirai et al 1984)
-
Vestibulospinal reflexes – appropriate tone for the neck and body muscles for the purpose of balance
-
-
Impaired kinaesthetic performance was found in people with dizziness/vertigo of cervical origin which may be as a result of lesioning or functional impairment of muscular and articular receptors, or by alteration in afferent integration and tuning (Heikkila et al 2000; Wyke 1979, Taylor & McCloskey 1988)
-
Altered kinaesthetic sensitivity has been implicated in functional instability of joints and their predisposition to re-injury, chronic pain and degenerative joint disease (Revel et al 1991, Hall et al 1995)
-
Postural control and voluntary eye movements were impaired during cervical restriction with a collar (Karlberg et al 1991)
-
Smooth pursuit and saccade abnormalities have been reported in people whiplash (mild – due to altered C/S proprioception {Oosterveld et al 1991}, severe – due to medullary lesions {Hildings et al 1989}), and in people suffering from fibromyalgesia with dysaesthesia (Rosenhall et al 1987)
-
62% of whiplash patients had at least 1 smooth pursuit abnormality at 2 years follow-up (Heikkila & Wenngren 1998)
-
Smooth pursuit was correlated with active ROM function of the C/S (Heikkila & Wenngren 1998; Karlberg et al 1991)
-
Vertigo was reported in 85% of whiplash subjects (Oosterveld et al 1991)
-
Whiplash subjects had less accurate ability to relocate their head in space after active displacement that turned their head away from the reference position (Heikkila & Astrom 1996) – esp. vertical mov'ts -> correlates with hyperflexion/extension injury
-
Signs & Symptoms of Cervical Vertigo
-
Correlating symptoms of imbalance with neck dysfunction
-
Cervical vertigo is characterised by a feeling of unsteadiness when standing and walking rather than rotatory vertigo (Brandt 1991)
-
Accompanied by pain – occipital, temporal, temporomandibular to orbital or forehead region
-
Tenderness on cervical palpation
-
Dizziness and nausea may be provoked by palpation of the lateral mass of the atlas (Scherer 1985)
-
Blurred vision, photophobia, direction-fixed, directional changing positional nystagmus, tinnitus, low frequency hearing loss
-
Imbalance may occur during the Unterberger stepping test
-
Correlating subjective findings (mechanism of onset, history of duration, frequency, area, and intensity) with physical and functional impairment is important in making a diagnosis and monitoring progression
-
Questionnaires
-
Activities Specific Balance Confidence Scale (ASBCS) (Powell & Myers 1995) & Dizziness Handicap Inventory (Tesio et al 1999)
-
Dynamic Gait Index (Shumway-Cook & Woollacott 2001) & Berg Balance Test (Berg et al 1992)
-
-
Cranial and carotid pulse and assessment for varicose veins
-
Complete neurological examination in all patients presenting with undiagnosed disorder of equilibration
-
Gait and balance and spontaneous nystagmus
-
Clinical test for Sensory Interaction in Balance (CTSIB) 'foam & dome test' - quiet standing eyes open/eyes shut, and again on foam for 15-30secs each (Shumway-Cook & Horak 1986) -
-
Posturography + vibration to the cervical extensors (illusion of lengthening) (Karlberg et al 1996) - measures the force applied by the patients feet
-
Assess dynamic visual activity – smooth pursuit neck torsion (SPNT) test, saccade tests, relocation error testing
-
VBI testing – positive predictive validity is zero, negative predictive value ranged from 63 – 97% (Cote et al 1996)
-
Unterberger stepping and Romberg quiet standing tests
-
Cervical Range of Motion testing ; extension stimulates the utricles
-
Adverse neural tension testing
-
Muscle and Joint Palpation – passive accessories, passive physiological
-
Shoulder, Scapula and thoracic spine
-
Head fixed body rotation manoeuvre - COR & CCR is activated without activation of the semicircular canals
-
Relocation testing using light on the head and moving into flexion/extension, and rotation - see above
Physical Assessment
-
Visual Disturbances
-
Smooth Pursuit Neck Torsion Test (SPNT) (Rosenhall et al 1996)
-
Tests the reflex interaction between smooth pursuit system and the proprioceptive system of the cervical spine
-
Velocity of eye movements relative to target object – net gain is calculated; abnormal result is reduced gain in the direction in which the head is rotated
-
When the body is rotated beneath a stationary neck a nystagmus can be induced
e.g. when the trunk is rotated left, the head is in relative right rotation, the COR helps the VOR to stimulate eye movements to the left in this position, but for teleologic reasons, in order to look forward, the saccadic system moves the eyes to mid point. The VOR with the aid of an overactive COR moves the eyes again to the left inducing a right-directional nystagmus (Tjell 1998, Tjell & Rosenhall 1998)
-
-
Dix – Hallpike manoeuvre for BPPV
The patient is in long sitting with the head rotated 45degrees to the side to be tested, then the patient is moved quickly into supine with the head in 30degrees of extension over a pillow under the rib cage, during which the eyes are observed for nystagmus for the posterior semicircular canals
85% of BPPV are upward rotating due to the posterior semicircular canals -
Cervicocephalic kinaesthetic sensibility (position sense + movement sense)
"kinaesthesia is a sensation which detects and discriminates between the relative weight of body parts, joint positions, and movements, including direction, speed and amplitude" (Newton 1982) -> the qualities that are supposed to be the result of proprioception-
Target matching is used to relocate the natural head posture (NHP) or to actively relocate a set point in range (Kristjansson et al 2003) in the transverse and saggital planes
-
Studies have demonstrated reduced relocation accuracy in whiplash patients (Heikkila & Wenngren 1998) but variable results in insidious neck pain (Kristjansson et al 2003)
-
60% sensitivity and 80% specificity (Kristjansson – unpublished work 2002)
-
Movements on the transverse plane stimulate mainly the semicircular canals, those in other planes stimulate the utricular otoliths which are sensitive to gravitational changes (Taylor & McCloskey 1990)
-
Slow movements test cervical proprioception due to the inertia of the cupula in the semicircular canals
-
An important aspect of proprioception is moment-to-moment feedback from tracking fast and unpredictable movements -> 'the fly' computer program with a Fastrak device is used for such determination (Kristjansson et al 2003, 2004)
-
Treatment
-
Positive affects have been reported for manipulative treatments (Cronin 1997, Galm et al 1998; Hulse et al 2000)
-
Both acupuncture and manipulation reduced dizziness/vertigo, neck pain and improved head repositioning error (Heikkila et al 2000)
-
Postural training with a significant eye-neck coordination component (Revel et al 1994) and vestibular component (Yardley et al 1998) have been shown to improve posture and dizziness
-
Multimodal approach advocated (Bracher et al 2000)
-
Recruitment of deep cervical flexors in neutral head and shoulder position (Jull 2000)
-
Loss of cervical lordosis in chronic whiplash patients (Kristjansson & Jonsson 2003) due to weak deep cervical flexors of the upper cervical spine (Jull 2000) and deep cervical extensors of the lower cervical spine (Kristjansson 2005)
-
Adequate movement control through range of motion
-
Determine whether global or segmental (upper, mid, low) stability has been lost
-
If segmental then try to move areas below and above the unstable segment keeping the latter stable – cognitive control
-
Next step is to recruit global and local stabilizers which most effectively move the dysfunctional segment under active control in a specific direction – the patient can be taught to only move the decontrolled segment through controlled ROM or move the whole cervical spine
-
The patient is specifically taught to control inner range and to move eccentrically from inner range to mid range and in some cases outer range (depending upon functional task which requires reinstating) (Kristjansson 2005)
-
There has been little research to the effectiveness of treatment strategies aimed at improving neuromuscular control and head carriage in the cervical spine
-
Revel et al (1994) conducted an 8 week eye-neck co-ordination exercise and awareness of movement with significant improvements in neck pain
Olafsdottir & Helgadottir (2001) conducted an 'awareness through movement' Feldenkreis program. After 4weeks significant improvements in NHP was detected (5.22deg + 1.79 vs 3.32 + 1.27 after treatment), additionally significant improvements in the Northwick Park Disability Index occurred using a 100mm VAS (Leak et al 1994)
-
-
Virtual reality systems to accommodate the need for 'systems' treatment eg. WiiFit, etc
-
Shock absorbing through the use of a trampoline
-
Eye-head coordination
-
Moving the eye balls with eyes open and shut,
-
visual tracking tasks with the head still,
-
gaze stability exercises whilst moving the head slowly and later progression to rapid movements,
-
keeping the gaze stability whilst moving in phase with the patients head in sitting, standing and walking, moving the trunk or varying the surface whilst maintaining the gaze on a fixed target
-
Balance exercises
-
Tandem stance on varying surfaces with eyes open/shut
-
Walking on the spot with eyes shut
-
Walking with saggital and transverse plane movements of the head and neck,
-
walking a distance and turning rapidly and walking back,
-
standing on a balance board making various head movements progressing to tracking a moving object,
-
walking on a treadmill detecting movements in the periphery without looking,
-
walking blindfolded
-
Task dependent exercises
-
Repeat the movement that makes one dizzy
-
General endurance exercise
Cognitive VOR training
-
Adaptation – resetting or retuning the VOR
-
-
Particularly good for unilateral lesions (hypofunction)
-
Must incorporate movement of the head and visual input
-
Takes time – requires 1-2 minutes practice with error signal
-
Context specific –need a wide range of frequencies i.e. head velocities and variety of positions - no distraction
-
-
Gaze Stabilization
-
Eye exercises – head still
-
Smooth pursuit – follow a moving object
-
Saccade – gaze redirection between 2 objects
-
Head exercises for VOR
-
Move head whilst focusing on stationary object 2m away
-
Eye-head exercises
-
Move eyes and head between 2 stationary objects (target must be something legible)
-
-
Substitution (useful for bilateral loss)
-
Physiological/Behavioural mechanisms
-
Sensory re-learning to change/substitute sensory strategies during functional tasks
-
Can bias strategies away from vertigo side or towards it use and drive compensatory processes
-
Body scan - teach client to attend to various inputs and switch back and forth to those
-
Remove or alter some inputs during a task e.g. eyes open/shut, foam, vibration, head tilts
-
Behavioural strategies as coping mechanisms
-
Learn how to move without triggering symptoms (if adaptation and habituation don't work)
-
Learn how to lessen the symptom experience via education, relaxation strategies
-
-
-
Habituation
-
Habituate repeated exposure to noxious stimulus to bring about neural changes to reduce sensitivity to the stimulus
-
Identify the source of conflicting sensory information i.e. vestibular, visual, somatosensory
-
Design movements based on those reproducing symptoms (1-4 movements, 2-3x each, 2-5x day)
-
Performed quickly enough through sufficient range to reproduce mild to moderate symptoms – increase this as habituation increases
-
Rest between each movement to allow symptoms to subside (approx. 1 minute)
-
May take up to 4weeks to notice changes
-
Do exercise for up to 2months intensively then gradually reduce them
-
Precautions in elderly with choice of movement
-
Physical and psychological factors predict outcome following whiplash injury
Pain Journal, 114, 141-148
Michele Sterling, Gwendolen Jull, Bill Vicenzino, Justin Kenardy and Ross Darnell
Predictors of outcome following whiplash injury are limited to socio-demographic and symptomatic factors, which are not readily amenable to secondary and tertiary intervention. This prospective study investigated the predictive capacity of early measures of physical and psychological impairment on pain and disability 6 months following whiplash injury. Motor function (ROM; kinaesthetic sense; activity of the superficial neck flexors (EMG) during cranio-cervical flexion), quantitative sensory testing (pressure, thermal pain thresholds, brachial plexus provocation test), sympathetic vasoconstrictor responses and psychological distress (GHQ-28, TSK, IES) were measured in 76 acute whiplash participants. The outcome measure was Neck Disability Index scores at 6 months. Stepwise regression analysis was used to predict the final NDI score. Logistic regression analyses predicted membership to one of the three groups based on final NDI scores (30 moderate/severe pain and disability). Higher initial NDI score (1.007-1.12), older age (1.03-1.23), cold hyperalgesia (1.05-1.58), and acute post-traumatic stress (1.03?1.2) predicted membership to the moderate/severe group. Additional variables associated with higher NDI scores at 6 months on stepwise regression analysis were: ROM loss and diminished sympathetic reactivity. Higher initial NDI score (1.03-1.28), greater psychological distress (GHQ-28) (1.04-1.28) and decreased ROM (1.03-1.25) predicted subjects with persistent milder symptoms from those who fully recovered. These results demonstrate that both physical and psychological factors play a role in recovery or non-recovery from whiplash injury. This may assist in the development of more relevant treatment methods for acute whiplash.
Development of motor system dysfunction following whiplash injury
Pain, Volume 103, Issue 1, Pages 65-73 (May 2003)
Michele Sterling, Gwendolen Jull, Bill Vicenzino, Justin Kenardy, Ross Darnell
Dysfunction in the motor system is a feature of persistent whiplash associated disorders. Little is known about motor dysfunction in the early stages following injury and of its progress in those persons who recover and those who develop persistent symptoms. This study measured prospectively, motor system function (cervical range of movement (ROM), joint position error (JPE) and activity of the superficial neck flexors (EMG) during a test of cranio-cervical flexion) as well as a measure of fear of re-injury (TAMPA) in 66 whiplash subjects within 1 month of injury and then 2 and 3 months post injury. Subjects were classified at 3 months post injury using scores on the neck disability index: recovered (30). Motor system function was also measured in 20 control subjects. All whiplash groups demonstrated decreased ROM and increased EMG (compared to controls) at 1 month post injury. This deficit persisted in the group with moderate/severe symptoms but returned to within normal limits in those who had recovered or reported persistent mild pain at 3 months. Increased EMG persisted for 3 months in all whiplash groups. Only the moderate/severe group showed greater JPE, within 1 month of injury, which remained unchanged at 3 months. TAMPA scores of the moderate/severe group were higher than those of the other two groups. The differences in TAMPA did not impact on ROM, EMG or JPE. This study identifies, for the first time, deficits in the motor system, as early as 1 month post whiplash injury, that persisted not only in those reporting moderate/severe symptoms at 3 months but also in subjects who recovered and those with persistent mild symptoms.
The relationship of cervical joint position error to balance and eye movement disturbances in persistent whiplash
Manual Therapy, Volume 11, Issue 2, May 2006, Pages 99-106
Julia Treleaven, Gwendolen Jull, Nancy LowChoy
Cervical joint position error (JPE) has been used as a measure of cervical afferent input to detect disturbances in sensori-motor control as a possible contributor to a neck pain syndrome. This study aimed to investigate the relationship between cervical JPE, balance and eye movement control. It was of particular interest whether assessment of cervical JPE alone was sufficient to signal the presence of disturbances in the two other tests. One hundred subjects with persistent whiplash-associated disorders (WADs) and 40 healthy controls subjects were assessed on measures of cervical JPE, standing balance and the smooth pursuit neck torsion test (SPNT). The results indicated that over all subjects, significant but weak-to-moderate correlations existed between all comfortable stance balance tests and both the SPNT and rotation cervical JPE tests. A weak correlation was found between the SPNT and right rotation cervical JPE. An abnormal rotation cervical JPE score had a high positive prediction value (88%) but low sensitivity (60%) and specificity (54%) to determine abnormality in balance and or SPNT test. The results suggest that in patients with persistent WAD, it is not sufficient to measure JPE alone. All three measures are required to identify disturbances in the postural control system. 
MRI study of the cross-sectional area for the cervical extensor musculature in patients with persistent whiplash associated disorders (WAD)
Manual Therapy, Volume 13, Issue 3, June 2008, Pages 258-265
James Elliott, Gwendolen Jull, Jon Timothy Noteboom, Graham Galloway
Cervical muscle function is disturbed in patients with persistent pain related to a whiplash associated disorder (WAD) but little is known about neck extensor muscle morphometry in this group. This study used magnetic resonance imaging to measure relative cross-sectional area (rCSA) of the rectus capitis posterior minor and major, multifidus, semispinalis cervicis and capitis, splenius capitis and upper trapezius muscles bilaterally at each cervical segment. In total, 113 female subjects (79 WAD, 34 healthy control; 18–45 years, 3 months–3 years post-injury) were recruited for the study.
Significant main effects for differences in muscle and segmental level were found between the two groups (P<0.0001) as well as a significant group * muscle * level interaction (P<0.0001). The cervical multifidus muscle in the WAD group had significantly larger rCSA at all spinal levels and in contrast, there were variable differences in rCSA measures across levels in the intermediate and superficial extensor muscles when compared to the healthy controls (P<0.0001). There were occasional weak, although statistically significant relationships between age, body mass index (BMI), duration of symptoms and the size of some muscles in both healthy control and WAD subjects (P<0.01).
It is possible that the consistent pattern of larger rCSA in multifidus at all levels and the variable pattern of rCSA values in the intermediate and superficial muscles in patients with WAD may reflect morphometric change due to fatty infiltrate in the WAD muscles. Future clinical studies are required to investigate the relationships between muscular morphometry, symptoms and function in patients with persistent WAD.
In vivo study of nerve movement and mechanosensitivity of the median nerve in whiplash and non-specific arm pain patients
Pain, Volume 115, Issue 3, Pages 248-253 (June 2005)
Jane Greening, Andrew Dilley, Bruce Lynn
Chronic pain following whiplash injury and non-specific arm pain (NSAP, previously termed diffuse repetitive strain injury) present clinicians with problems of diagnosis and management. In both patient groups there are clinical signs of altered nerve movement and increased nerve trunk mechanosensitivity. Previous studies of NSAP patients have identified altered median nerve movement at the wrist. The present study uses high frequency ultrasound imaging to examine changes to median nerve movement and clinical examination to assess altered mechanosensitivity of the median nerve. Longitudinal median nerve movement was measured in the forearm during maximal inspiration in nine post-whiplash patients with chronic neck and arm pain and eight controls subjects. Eight NSAP patients and seven controls were also studied. Transverse median nerve movement at the proximal carpal tunnel during 30° wrist extension to 30° flexion was also measured. A clinical examination of nerve trunk allodynia was performed in all subjects. Longitudinal nerve movement in the forearm was reduced by 71% in the post-whiplash patients and by 68% in NSAP patients compared to controls. In the whiplash patients the pattern of transverse median nerve movement at the proximal carpal tunnel was significantly different to controls (patient mean=2.57±0.80mm (SEM) in a radial direction; control mean=0.39±0.52mm in an ulnar direction). Signs of neural mechanosensitivity (i.e. painful responses to median nerve trunk and brachial plexus pressure and stretch) were apparent in both patients groups. Change in nerve tension and neural mechanosensitivity may contribute to symptoms in whiplash and NSAP patients.
Reduced reactivity and enhanced negative feedback sensitivity of the hypothalamus-pituitary-adrenal axis in chronic whiplash-associated disorder
Pain, Volume 119, Issues 1-3, 15 December 2005, Pages 219-224
Jens Gaab, Susanne Baumann, Angela Budnoik, Hanspeter Gmünder, Nina Hottinger, Ulrike Ehlert
Dysregulations of the hypothalamus–pituitary–adrenal (HPA) axis have been discussed as a physiological substrate of chronic pain and fatigue. The aim of the study was to investigate possible dysregulations of the HPA axis in chronic whiplash-associated disorder (WAD). In 20 patients with chronic WAD and 20 healthy controls, awakening cortisol responses as well as a short circadian free cortisol profile were assessed before and after administration of 0.5 mg dexamethasone. In comparison to the controls, chronic WAD patients had attenuated cortisol responses to awakening, normal cortisol levels during the day, and showed enhanced and prolonged suppression of cortisol after the administration of 0.5 mg dexamethasone. Dysregulations of the HPA axis in terms of reduced reactivity and enhanced negative feedback suppression exist in chronic WAD. The observed endocrine abnormalities could serve as a systemic mechanism of symptoms experienced by chronic WAD patients.
Systemic Immune Response in Whiplash Injury and Ankle Sprain: Elevated IL-6 and IL-10
Clinical Immunology, Volume 101, Issue 1, October 2001, Pages 106-112
Jouko Kivioja, Volkan Özenci, Luciano Rinaldi, Mathilde Kouwenhoven, Urban Lindgren, Hans Link
Whiplash injury and whiplash-associated disorders (WAD) are significant problems of modern society. Numerous attempts have been made to characterize the nature of whiplash injury. Whether the immune system is involved during the disease process is not known. In a prospective study, using enzyme-linked immunospot (ELISPOT) assays, we examined numbers of blood mononuclear cells (MNC) secreting pro- (IFN-?, TNF-a, IL-6) and anti-inflammatory (IL-10) cytokines in patients with WAD and, for reference, patients with ankle sprain and multiple sclerosis and healthy subjects. An immune response reflected by elevated numbers of TNF-a- and IL-10-secreting blood MNC was observed in patients with WAD examined within 3 days compared to 14 days after the whiplash injury. The patients with WAD examined within 3 days after the injury had also higher numbers of IL-6 and IL-10 secreting blood MNC compared to healthy subjects. The alterations of cytokine profiles observed in WAD were also observed in patients with ankle sprain when examined within 3 days after trauma. In contrast, there were no differences for cytokine profiles between patients with WAD examined 14 days after the whiplash injury and healthy subjects. Relatively minor trauma like WAD and ankle sprain are associated with a systemic dysregulation in numbers of cells secreting pro- as well as anti-inflammatory cytokines.
Women experience greater heat pain adaptation and habituation than men
Pain, Volume 145, Issue 3, Pages 350-357 (October 2009)
Javeria A. Hashmi, Karen D. Davis
It is not clear how males and females cope with pain over time and how sensory and emotional qualities fluctuate from moment to moment, although studies of pain at discrete time points suggest that women are more pain sensitive than men. Therefore, we developed a new broader-based pain model that incorporates a temporally continuous assessment of multiple pain dimensions across sensory and affective dimensions, and normalized peak pain intensity to unmask sex differences that may otherwise be confounded by inter-individual variability in pain sensitivity. We obtained continuous ratings of pain, burning, sharp, stinging, cutting, and annoyance evoked by repeated prolonged noxious heat stimuli in 32 subjects. Strikingly, females reported more pain than males at the outset of the first exposure to pain, but then experienced less pain and annoyance than males as a painful stimulus was sustained and with repeated stimulation. Patterns of pain and annoyance attenuation in women resembled the attenuation of sharp, stinging and cutting sensations, whereas patterns of pain and annoyance in men resembled burning sensations. Taken together, these data demonstrate a prominent sex difference in the time course of pain. Notably only females demonstrate adaptation and habituation that allow them to experience less pain over time. These findings suggest a sexual dichotomy in mechanisms underlying pain intensity and annoyance that could involve specific quality-linked mechanisms. Importantly, temporal processing of pain differs between males and females when adjusted for sex differences in pain sensitivity. Our findings provide insight into sex differences in tonic and possibly chronic pains.
Pain, perceived injustice and the persistence of post-traumatic stress symptoms during the course of rehabilitation for whiplash injuries
Pain, Volume 145, Issue 3, Pages 325-331 (October 2009)
Michael J.L. Sullivan, Pascal Thibault, Maureen J. Simmonds, Maria Milioto, André-Philippe Cantin, Ana M. Vellya
The present study assessed the role of pain and pain-related psychological variables in the persistence of post-traumatic stress symptoms following whiplash injury. Individuals (N=112) with whiplash injuries who had been admitted to a standardized multidisciplinary rehabilitation program were asked to complete measures of pain, post-traumatic stress symptoms, physical function and pain-related psychological variables at three different points during their treatment program. The findings are consistent with previous research showing that indicators of injury severity such as pain, reduced function and disability, and scores on pain-related psychological were associated with more severe post-traumatic stress symptoms in individuals with whiplash injuries. Contrary to expectations, indicators of pain severity did not contribute to the persistence of post-traumatic stress symptoms. Univariate analyses revealed that self-reported disability, pain catastrophizing and perceived injustice were significant determinants of the persistence of post-traumatic stress symptoms. In multivariate analyses, only perceived injustice emerged as a unique predictor of the persistence of post-traumatic stress symptoms. The results suggest that early adequate management of pain symptoms and disability consequent to whiplash injury might reduce the severity of post-traumatic stress symptoms. The development of effective intervention techniques for targeting perceptions of injustice might be important for promoting recovery of post-traumatic stress symptoms consequent to whiplash injury.
Influences on the fusimotor-muscle spindle system from chemosensitive nerve endings in cervical facet joints in the cat: possible implications for whiplash induced disorders.
Thurnberg et al (2001) Pain, 91, 15-22
Randomized controlled trial of exercise for chronic whiplash-associated disorderStewart et al (2007), Pain, Volume 128, Issue 1, Pages 59-68Whiplash-associated disorders are common and incur considerable expense in social and economic terms. There are no known effective treatments for those people whose pain and disability persist beyond 3 months. We conducted a randomized, assessor-blinded, controlled trial at two centres in Australia. All participants received 3 advice sessions. In addition the experimental group participated in 12 exercise sessions over 6 weeks. Primary outcomes were pain intensity, pain bothersomeness and function measured at 6 weeks and 12 months. Exercise and advice was more effective than advice alone at 6 weeks for all primary outcomes but not at 12 months. The effect of exercise on the 0–10 pain intensity scale was -1.1 (95%CI -1.8 to -0.3, p=0.005) at 6 weeks and -0.2 (0.6 to -1.0, p=0.59) at 12 months; on the bothersomeness scale the effect was -1.0 (-1.9 to -0.2, p=0.003) at 6 weeks and 0.3 (-0.6 to 1.3, p=0.48) at 12 months. The effect on function was 0.9 (0.3 to 1.6, p=0.006) at 6 weeks and 0.6 (-0.1 to 1.4, p=0.10) at 12 months. High levels of baseline pain intensity were associated with greater treatment effects at 6 weeks and high levels of baseline disability were associated with greater treatment effects at 12 months. In the short-term exercise and advice is slightly more effective than advice alone for people with persisting pain and disability following whiplash. Exercise is more effective for subjects with higher baseline pain and disability. Habituation of the early pain-sensitivity respiratory response in sustained pain. |
Kato et al (2001) Pain, 91, 57 - 63
|
References
Anthony, M.,(1989). Unilateral Migraine or Occipital Neuralgia?.In: Clifford, R.,F.,(1989) (ed.). New Advances in Headache Research. London. Smith-Gordon. 39 to 43.
Bakker & Richmond (1982). Muscle spindle complexes in muscles around the upper cervical vertebrae in the cat. J. Neurophysiol, 48, 62 to 74
Bogduk, N.,(1983). The anatomy and mechanism of cervical headaches. Proceedings of cervical headache symposium. Manipulative Therapists'Association of Australia, Sydney, July, 9 to 24.
Bogduk, B., Corrigan, B., Kelly, P., Schneider, G., Farr, R., (1985). Cervical Headache. The Medical Journal of Australia, 143, 202, 206 to 7.
Bogduk, B., (1992). The Anatomical Basis for Cervicogenic Headache. Journal of Manipulative and Physiological Therapeutics, 15, 1, 67 to 70.
Djupsjoebacka, M (2008) Proprioception and Neck/Shoulder pain. In Fundamentals of Musculoskeletal Pain, Graven-Nielsen & Arendt-Nielsen, Eds, Ch 24, IASP Press, Seattle.
Edeling, J.,(1982). The true cervical headache. South African Medical Journal,62, 531 to 534.
Falla et al (2007) Effect of neck exercises on sitting posture in patients with chronic neck pain. Phys Ther, 87, 408 to 417
Falla D (2008) Neck pain and neuromuscular control. In Fundamentals of Musculoskeletal Pain, Graven-Nielsen & Arendt-Nielsen Eds, IASP Press Seattle Ch 26
Fitz-Ritson D (1995). Phasic exercises for cervical rehabilitation after 'whiplash' trauma. J Manipulative Physiol Ther, 18, 21 to 24
Goadsby, P.,J.(1993). The anatomy and physiology of the cerebral circulation in relationship to the assessment and management of headache. 7th World Congress on Pain I.A.S.P ..Paris, France.
Gawel, M.,J., Rothbart, P., J., (1992). Occipital nerve block in the management of headache and cervical pain. Cephalgia, 12, 9 to 13.
Guez et al (2003) Chronic neck pain of traumatic and non-traumatic origin: a population-based study. Acta Orthop Scand, 74, 576 to 579
Jarus T (1994). Motor learning and occupational therapy: the organization of practice. Am J Occup Ther, 48, 810 to 816
Johansson et al (1995). A method for analysis of encoding of stimulus separation in ensembles of afferents. J Neurosci Methods, 63, 67 to 74
Jull GA (2000). Deep cervical flexor muscle dysfunction in whiplash. J Muasculoskeletal Pain, 8, 143 to 154
Jull, G., Bogduk, N., Marsland, A.,(1988). The Accuracy of Manual Diagnosis for Cervical Zygapophysial Joint Pain Syndromes. The Mendical Journal of Australia, 148, 233 to 236.
Jull et al (2007a). Cervical musculoskeletal impairment in frequent musculoskeletal headache. Part 1: Subjects with single headaches. Cephalgia, 27, 793 to 802
Jull et al (2007b). Retraining cervical joint position sense: the effect of two exercise regimes. J. Orthop. Res., 25, 404 to 412
Kadi et al (2000). The effects of different training programs on the trapezius muscle of women with work related neck and shoulder myalgia. Acta Neuropathol (Berl), 100, 253 to 258
Karlberg et al (1991). Effects of restrained cervical obility on voluntary eye movements and postural control. Acta Otolaryngol, 111, 664 to 670.
Kelly, P.,(1978). Manipulative Therapy in the Treatment of Migraine. In: Proceedings of Manipulative Therapy Association of Australia: Inaugral Congress. Sydney. Australia.
Kelly, P.,(1983). The Management of Cervical Headache. In: Proceedings of Cervical Headache Symposium. M.T.A.A. Sydney. Australia.
Lee et al (2006) Test-retest reliability of cervicocephalic kinesthetic sensibility in three cardinal planes. Man Ther, 11, 61 to 68
Liu-Chen, L.,-Y., Mayberg, M.,R., Moskowitz, M.,R.,(1983). Immunohistochemical evidence for a substance P containing trigeminovascular pathway to pial arteries in cats. Brain Research , 268, 162 to 166.
Lundblad et al (1999). Randomized controlled trial of physiotherapy and Feldenkrais interventions in female workers with neck-shoulde compliants. J Occup Rehabil, 9, 179 to 194
Maitland, G.,D.,(1986). Vertebral Manipulation (5th ed ). London. Butterworth & Co..
Olesen, J.,(1993). The Classification and Diagnosis of Headache Disorders. 7th World Congress on Pain. I.A.S.P. Paris. France.
Parker, G., B.,Tupling, H., Pryor, D.,S.,(1978). A Controlled Trial of Cervical Manipulation for Migraine. Australian and New Zealand Journal of Medicine,8, 589 to 593.
Parker, G.,B., Pryor D.,S.,Tupling, H.,(1980) Why Does Migraine Improve During a Clinical Trial? Further Results from a Trial of Cervical Manipulation for Migraine. Australian and New Zealand Journal of Medicine, 10, 192 to 198.
Pedersen et al (1998). Alterations in information transmission in ensembles of primary muscle spindle afferents after muscle fatigue in heteronymous muscle. Neuroscience, 84, 953 to 959
Pfaffenrath, V., Dandekar, R., Pollman, W. (1987). Cervicogenic headache-the clinical picture, radiological findings and hypothesis on its pathophysiology. Headache,27, 495 to 9
Sjaastad, O., Stovner, L.,J.,(1993). The IHS Classification For Common Migraine. Is It Ideal? Headache,33 , 372-375.
Taimela et al (2000) Active treatment of chronic neck pain: a prospective randomized intervention. Spine, 25, 1021 to 1027
Treleaven et al (2003) Dizziness and unsteadiness following whiplash injury: characteristic features and relationship with cervical joint positioning error. J Rehab Med 35, 36 to 43
Treleaven et al (2005a). Smooth pursuit neck torsion test in whiplash associated disorders: Relationship to self reports of neck pain and disability, dizziness, and anxiety. J Rehab Med, 37, 219 to 223
Treleaven et al (2005b). Standing balance in persistent whiplash: a comparison between subjects with and without dizziness. J Rehab Med, 37, 224 to 229
Vernon, H., Steinman, I., Hagino, C.,(1992). Cervicogenic Dysfunction in Muscle Contraction Headache and Migraine: A Descriptive Study. Journal of Manipulative and Physiological Therapeutics, 15, 7, 418 to 427.
Zusman, M., (1992). Central Nervous System Contribution to Mechanically Produced Motor and Sensory Responses. Australian Journal of Physiotherapy, 38, 4, 245 to 255.
Zusman, M., (1994). The Meaning of Mechanically Produced Responses. Australian Journal of Physiotherapy, 40, 1,35 to 39.
peripheral sympathetic nervous system and WDR hypersensitivity
link to neurophysiology and PET scan of cortex
Last update : 21 February 2017
 What We do
What We do What We Treat
What We Treat



















































































































