



Introduction
Knee injuries are of 2 forms, traumatic and atraumatic (repetitive strains). Traumatic injuries include those from fast 'cutting and turning' movements as seen in soccer and skiing. Essentially an inward motion of the knee relative to the foot and hip. These injuries can include the classic 'triad' of anterior cruciate ligament (ACL), medial meniscus and medial collateral ligament.
The knee and it's neighbouring 'ball and socket' joints and SIJ dysfunction contributing to knee injuries
Have you considered the control over the knee occurring from ball & socket joints? Traditionally, anatomical constructs of reasoning suggest that the lateral & medial stability of the knee is precariously maintained by collateral ligaments. However, what controls the tibia and femur? Since, the hip and talo-navicular (foot) joints are ball & socket joints, they serve the function of providing a large range of movement (ROM). The motor control conundrum that such large ROM presents is it's balance with stability not only in the hip and talonavicular joint but also those regions abilities to contribute to the protection of the (patella) knee cap and ligaments of the knee. Indeed, lumbopelvic landing kinematics and EMG demonstrated increased muscular activity and medial knee displacement on single leg step down in women with reduced gluteal hip strength (Popovich & Kulig, 2012, Med Sc Ex Sp, 44, 1, 146-153). Excessive internal rotation in the hip has also been shown to increase the shear stress on the indersurface of the patella (knee cap) (Liao et al 2016, Med Sc Sp Ex, 47, 9, 1775-1780). Reduced gluteal strength may be, amongst other things, the direct result of pain occasioned by a counternutated sacroiliac joint (SIJ) caused by forward displacement of the head of femur from an over active adductor muscle. Obturator nerve biomechanics, innervated by the L2-L4, should also be considered during the clinical reasoning process.
Increased muscle tension in the adductor muscles can result in an anterior shift of the head of the femur, which is countered by increased iliacus activity resulting in anterior rotation of the innominate, with consequent counternutation and instability of the SIJ. Hereby, the pre-existing tension of the adductor muscle dictates that it's primacy results in it as becoming the prime mover regardless of the direction of movement!!
Motor Control
Areas of increased ROM need to have a counterbalancing co-ordinated system of dynamic stability. Models of motor control have used analogies of a mass on a coil spring pertubating around a fixed point. Such oscillations of movement are typical of common movements in our daily lives, such as walking, running, swimming, etc. Inherent to our rehabilitation models and models of prophylactic training suggest that exercises need to engage oscillations in controlled movement.

link to theoreticl explanation can be found in the Shoulder section of this site
Inverse Dynamics
Models of inverse dynamics reveal that accelerating body parts will have a counter accelerating conservation of energy component in them, whereby momentum is captured by elongating soft tissue structures such as tendons and eccentric muscle contractions countered by elastic 'rebound' shortening of tendons and concentric contractions of muscles. It should be noted that the initial phase of concentric contraction actually momentarily accelerates soft tissue elongation just before the rebound. The water content contained within tendons along with the collagen scaffolding prevents the tendon from pulling apart. As we age, tendons become 'drier' which is worsened with poor diet and inactivity.
Motor learning theory devised by Bernstein suggests that the body will use the momentum of the limbs to optimize the degrees of freedom in the system. Similar to a mass-spring analogy where the perturbations of the mass will be dependent on the damping characteristics of the spring, the brain will introduce muscle tone to dampen the angular velocity and hence acceleration of the system. Therefore, instead of the muscles of the leg lifting the limb, the antagonistic muscles are decelerating the limb towards the end of trajectory. Moreover, by using eccentric (muscle lengthening and contracting) muscle contractions the system becomes efficient through these decelerating movements through enhanced visco-elastic rebound as well as the conservation of momentum.
see Motor Learning section for further explanations
Exercises
As such, the muscles around the hip and talo-navicular joints perform the function of multidimensional stability. Clearly, the femur affects knee positioning and the position of the ilium/hip will affect timing of the muscles around the hip-thigh. Any anterior ilial rotation generally makes it difficult for the gluteus maximus to fire before or simultaneously with the hamstring muscles. Tightness of the adductor muscle can cause an 'inflare' of the ilium, potentially placing adverse tension on the ischiococcygeal and sacrotuberal ligaments. Moreover, this adverse tension of the adductors could affect the nutrition to the knee through the phylogenetic link of these muscles with the medial collateral ligament and hence medial meniscus. Any adverse function of the iliopsoas can affect femoral blood flow which is likely to affect slow twitch, stabilising, endurance muscles more than fast twitch, glycolitic, ballistic muscles. Hence, as the duration of activity increases, movement stability may break down, leading to 'poor form' and potential injury.
Strengthening of the hip abductor and lateral rotator muscles associated with functional training results in improved lower limb dynamic alignment and increses the strength and functional performance in women (Baldon et al, 2012, Med Sc Sp Ex, 44, 1, 135-145). These exercises included non-weight bearing and core exercises with the pelvis and spine maintained in neutral during
phase 1 : (wks 1- 3) aim to enhance motor control and endurance of the transverse abdominus, multifidus, hip abductors and lateral rotators
- in side lying hip abduction and lateral rotation
- in prone hip extension and lateral rotation with knee flexed
- in quadruped hip lateral rotation/abduction/extension
- in side lying 'the clam' with theraband around the knees
- single leg stance on unstable platform such as a wobble board
- seated swiss ball
3 sets of 12 repetitions and 120 seconds rest between series.
Phase 2 : (wks 3-5) aim to increase strength of the hip abductors, lateral rotators, as well as the knee flexors and extensors
- modified side ways plank (on knees)
- modified plank (on knees)
- single leg standing and arm resistance extension training with theraband
- single leg standing and arm resistance training with theraband into trunk rotation
- single leg stance on unstable platform whilst catching and throwing a ball
- hip hitches with weight around ankle
Phase 3 : (wks 5-8) aim to learn proper lower limb alignment during functional activities
- full side ways plank
- full prone plank
- kneeling on swiss ball
- lunge with lateral resistance around knee with theraband
- half lunge off step
- full lunge off step with lateral resistance using theraband
Examination
The examination process requires the establshment of the characteristics of the disorder and whether it was a result of 'misuse', 'abuse', 'disuse' or 'overuse'. In traumatic injuries it is important to ascertain the 'mechanism of injury" and it subsequent consequences, trying to establish a 'timeline' of injury and recovery. Also it is important to gain an understanding as to the past history of knee injuries as well as injuries to adjacent areas such as the hip, pelvis, back and foot. The subjective examination should include questions which allow the therapist to make a precise decision on the stage, stability, irritability and severity of the disorder. In atraumatic conditions, the timeline of symptoms need to be understood in order to establish 'cause and effect', thereby being able to prioritise the treatment in order of importance.
Physical Examination
The physical examination should include analysis of
- gait
- pelvc symmetry
- lumbo-pelvic dynamics
-
Abdominal and Gluteal Strengthening
- ROM's of the hip, knee, foot and L/S
- Muscle energy techniques
- Taping of the patella
- femoral pulse
- inferior lateral movements of the T/S and lateral diaphragm control over Psoas Major function

-
foot dynamics (esp. pronation supination)
-
go to foot - orthotics section for further details
-
Hip - lumbopelvic control
- Relationship between the deep and superficial abdominal muscles and their affect on pelvic symmetry and lumbopelvic rhythm.
Connell AT (2008) Concepts for assessment and treatment of anterior knee pain related to altered spinal and pelvic biomechnics: a case report. Manual Therapy, 13, 560-563
This author used 3 sessions of treatment to the T10/11, T11/12, T12/L1 and L5/S1 to improve the ROM and ability to squat in a patient with anterior knee pain.
Grindstaff TL et al (2009) Effects of lumbopelvic joint manipulation on quadriceps activation and strength in healthy individuals. Manual Therapy, 14, 415-420.
Green A and Perry (2008) An investigation into the effects of a unilaterally applied lumbar mobilisation technique on peripheral sympathetic nervous system activity in the lower limbs. Manual Therapy, 13, 492-499.
These investigators examined 45 healthy naive males and performed a unilateral Posteroanterior technique to the zygopophyseal joint of L4/5 and recorded skin conductance in the lower limb using a randomized control trial. They found mobilsations at 2Hz resulted in side-specific peripheral SNS changes in the lower limbs. In their review they suggested that it is the oscillatory component of the mobilisation which has the greatest effect on the SNS (Gebber et al 1999, Kenny et al 1991, McGuiness et al 1997). The effect reported was 13.5% (+/- 20.25). Proposed mechanisms were direct stimulation of the SNS ganglion, soft tissue joint receptor reflexes, myogenic reflexes and descending modulatory responses.

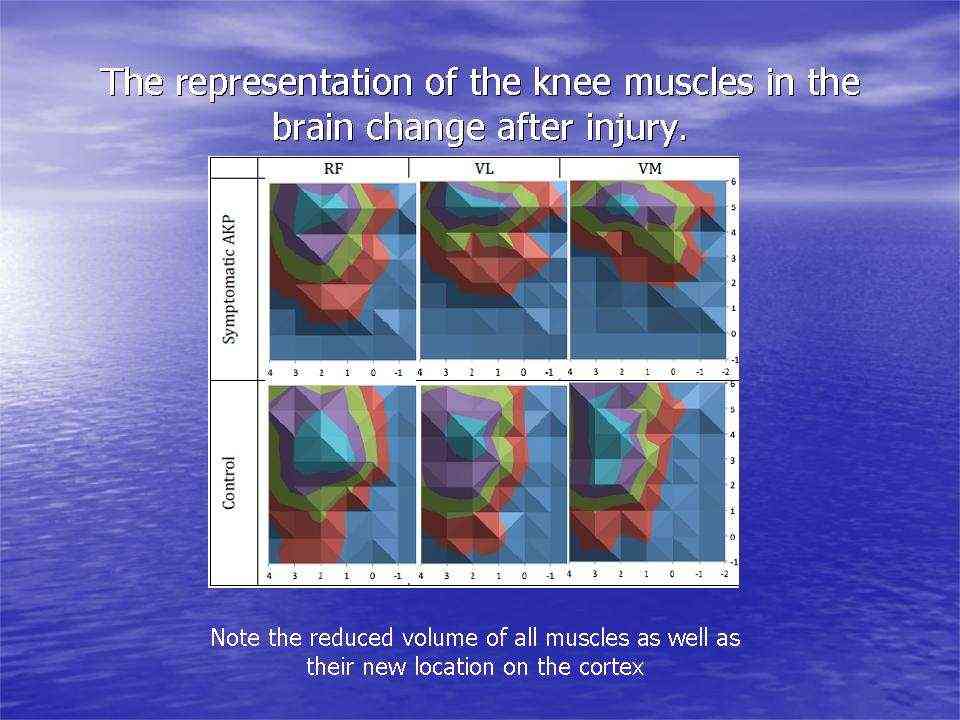
Cortical changes in knee muscle representation after injury
Investigations in Australia looking at 40-50 year old women with chronic knee pain, demonstrated the significant reduction in the volume of muscle representation in the cerebral cortices, as well as changes in the location of these muscle representations. Moreover, where neurons who 'fire together, wire together' it would be of utmost importance to find exercises that act as functional synergies and relate in a real or a 'virtual' manner to the environmental context in which they need to fire. This also becomes particularly important in psychological behavioural issues of 'fear avoidance' and disuse atrophy. Ideally rehabilitation stimulates 'wiring and firing together' of goal oriented regions of the brain rather than those which are directed at fearing and avoiding movement. Therapist must instill confidence through their choices of treatment whereby they outline and hence monitor the expectations of outcome.
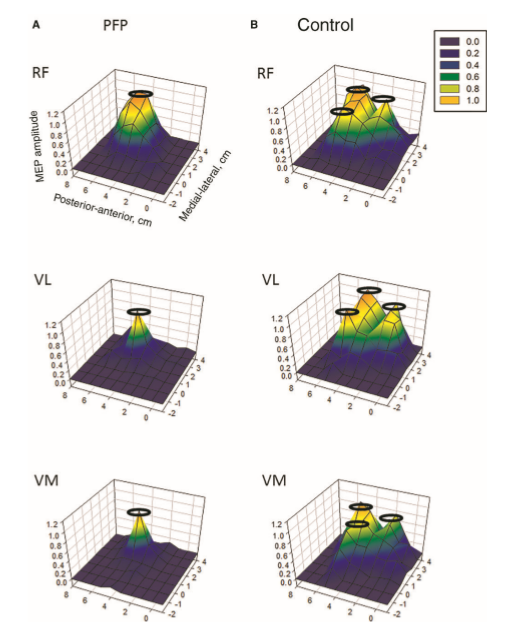
Cortiical representation in Patellofemoral Pain (PFP). Te et al (2017) Pain Medicine, 0, 1-11
Transcranial magnetic stimulation analysis of knee representation in the brain pre/post injury. (Abrahao Fontes Baptista 2014)
EMG
Problems of the patellofemoral joint (anterior knee pain) in which the ability to produce knee extensor torques are reduced and the knee muscle EMG activity is eratic has been shown by Rathleff et al 2013 (Med Sc Sp Ex, 45, 9, 1730-1739). Training using EMG biofeedback can be an important aspect in knee rehabilitation. Frequently, the balance between VMO (Vastus Medialis - inside knee muscle) and VL (vastus lateralis - outside knee muscle) is examined and trained. However, EMG biofeedback can also be used in combination with transverse abdominis, gluteus medius, medial calf muscle training.

Strengthening and Lengthening
Iliotibial Band lengthening and combined gluteal/quads/abdominal strengthening

Treatment should include techniques and exercises which ameliorate the problems identified during the examination. These may include muscle energy techniques (MET), soft tissue massage (STM), dry needling (intramuscular stimulation {IMS}), myofascial release, EMG biofeedback, taping, joint mobilisations, and motor learning principles.
Patella Tracking Dysfunction

Similarly, to what was described above with ligamentous injuries, one needs to consider the influence of the pelvis in patella tracking dysfunction. If the pelvis has an adductor longus with high tone then this could rotate the hemi-pelvis inwards on the stance leg. Subsequently tension is generated in the lateral rotators of the hip (eg obturator internis and externis) which could irritate the obturator nerve creating further spasms in the adductor longus. This in turn may generate shearing across the pubic symphysis resulting in pain in the groin. Additionally, the rotation &/or inflare of the hemipelvis may result in anterior ilial rotation (counter-nutation) creating an irritated rectus femoris and ITB/Tfl. Furthermore, this counternutation may place excessive strain through the biceps femoris resulting in sacrotuberal and sacroiliac ligament irritation.
Patella Muscle Taping
Knee taping has been shown to influence the viscoelastic properties of muscles hereby improving the shock absorbing capacity of the muscles around joints. Through the use of elastography, an investigation by Hug et al (2014) is the first study to support the hypothesis that deloading tape reduces stress in the underlying muscle region, at rest and during contraction, thereby providing a biomechanical explanation for the effect observed during rehabilitation in clinical practice (reduce pain, restore function, and aid recovery). Medicine & Science in Sports & Exercise: December 2014 - Volume 46 - Issue 12 - p 2317–2325

Taping or other aids can also be used around the hip/buttocks to prevent femur internal rotation thereby reducing the relative lateral alignment of the patella w.r.t the femur.
Functional Knee Exercises
Cartilage (meniscus) injuries
People frequently ask whether they can resume activities such as running after partial menisectomy. The bad news is that the effect of long-term vigorous physical activity on healthy adult knee cartilage is dependent upon bone marrow lesions (Teichtahl et al 2011, Med Sc Sp Ex, 44, 6, 985-992). Since the healthy meniscus protects the articular bone, then partial meniscectomy may lead to altered articular biomechanics predisposing to early onset of osteoarthritis due to a predisposing bone marrow lesion. Hence, it may be better for the runner in their 50's to take up cycling. Alternatively, depending upon the intensity and volume of exercise regular MRI's may be required, to establish the presence of are any bone marrow lesions, as cartilage thickness does not seem to be a good predictor of joint degeneration, in the early to medium stages of pathology.
Degenerative changes in the knee
Researchers have shown that progressively implemented high impact intensive exercise creates enough stimuli and exerts favorable effects on patella cartilage quality and physical function in postmenopausal women with mild knee OA (Koli et al 2016, Med Sc Ex Sp, 47, 9, 1767-1774).
Case Presentations
Conclusion
The examination and treatment of the knee should include assessment of all the structures, including those joints and structures above and below the knee, which can affect knee function. Prior to the physical examination, a thorough subjective examination should be conduct to enable the client and the therapist to engage in the clinical reasoning process. Interested readers should look at the Instructional Design section of this website.

Last update : 16 October 2017
 What We do
What We do What We Treat
What We Treat



















































































































