



by Martin Krause

Introduction
Knee injuries are quite prevalent in soccer. Injuries can be separated into 'contact' and 'non-contact' injuries. Non-contact injuries include the 'triad' of the inside cartilage (medial meniscus) damage, along with the medial collateral ligament (connecting the two bones on the inside) and anterior cruciate ligament (ACL). There appears to be a higher prevalence of this injury in young women. Indeed, increased susceptibility to ACL injuries has been found in adolescent girls with reduced hamstring strength, who also have also been shown to have reduced hip abduction strength (Wild et al 2013, Medicine & Science in Sports & Exercise, 45, 3, 497–505). However, several health benefits have been identified with the participation in soccer, amongst which have even included significant reductions in blood pressure in middle aged hypertensive men (systolic and diastolic blood pressures decreased (P < 0.01) over 6 months from 151 ± 10 to 139 ± 10 mm Hg and from 92 ± 7 to 84 ± 6 mm Hg) (Krustrup et al 2013, Medicine & Science in Sports & Exercise, 45, 3, 553–561). Additional benefits include psychological ones representing aspects such as 'a sense of belonging' which occurs through socialisation. Moreover, individual psychological traits will influence a persons responses as they go through the 'stages' of injury and recovery.


Interestingly, high specialisation in female youth soccer players is associated with the increased likelihood of sustaining a serious injury (Xiao et al 2021, Med Sc Sp Ex, 53, 10, 2086-2092).Current youth soccer players are specialising earlier and committing to play college soccer at a younger age compared with when current college and professional soccer players did. Suggestions are that a youth soccer player shouldn't spend more hours training per week than their age. Additionally, issues of 'burn out' may also occur.
Biomechanics of the Knee
Investigations have shown that as the knee transitions to weight bearing at low knee flexion angles (15-30º), there is anterior (forward) translation of the tibia (shin bone) to the femur (thigh bone), which is normally restrained by the ACL (Schultz et al 2011 Med Sc Sp Ex, 43, 2, 287-295). These knee flexion angles are a common angle for aspects of soccer such as kicking, dribbling and fast sideways 'cutting' actions. Moreover, during side step cutting action, females have been shown to exhibit 20% higher knee adductor moments and nearly twice the knee valgus when compared with males (Sigward et al 2012, Med Sc Sp Ex, 44, 8, 1497-1503). Additional problems may include patellofemoral (anterior knee) pain in which the ability to produce knee extensor torques are reduced and the knee muscle EMG activity is erratic (Rathleff et al 2013, Med Sc Sp Ex, 45, 9, 1730-1739)
Mechanism of injury
These injuries usually occur as a result of a fast movement with a degree of rotation and pivoting involved. The foot and lower leg turn outward, relative to the upper leg turning inward, creating a gapping force on the inside of the knee. This is commonly referred to as a valgus force. People with poor hip control are thought to be more vulnerable to an uncontrolled valgus force. The combination of knee valgus strain (51Nm) and hip internal rotation strain (25.9Nm) has been demonstrated to increase the strain on the ACL by 0.115, high enough to cause it to rupture (Shin et al 2011, Med Sc Sp Ex, 43, 8, 1484-1491), as the rupture strain lies between 0.09 -> 0. Additionally, in females with abnormal hip kinematics, femoral (thigh - hip) internal rotation has been demonstrated to increase patellofemoral (knee cap) hydrostatic pressure and octahedral shear stress (Liao et al 2016, Med Sc Ex Sp, 47, 9, 1775-1780)
Contrasting hip strength and control during landing in women.
It has been shown that individuals with reduced hip strength have greater pelvic angular displacement, peak velocity, total angular excursion and higher muscle activation of the trunk and gluteal muscles than stronger individuals (Popovich & Kulig 2012 Med Sc Sp Ex, 44, 1,146-153). Lack of control of the inward movement of the knee has been demonstrated to improve with functional hip abductor and external rotator training (Baldon et al 2012 Med Sc Sp Ex, 44, 1, 135-145). They also employed core stabilising exercises for the abdominal region. However, static core stabilising exercises have not been shown to improve knee loading (Jamison et al 2012, Med Sc Sp Ex, 44, 10, 1924-1934). Therefore, dynamic trunk exercises using perturbations of movement need to be incorporated into a rehabilitation program. Pelvic floor exercises are also recommended by us as the obturator internis muscle is a hip lateral rotator whose myofascial membrane is continuous with the pelvic floor.
Researchers have found ongoing deficits in dynamic strength after ACL reconstructions. Specifically, a 12% deficit in single hop, 21% deficit in triple hop, and 17% deficit on cross-over hop test relative to healthy individuals. In addition the average hop test results were well below suggested clinical cut-offs for people returning to sport (Peebles et al 2019, Med Sc Sp Ex, 51, 4, 624-629). Such deficits may affect the risk of future injury. Additionally, reduction in peak loading capacity may influence cartilage regeneration, as demonstrated by MRI of compositional changes to the tibiofemoral cartilage (Pfeiffer et al 2019, Med Sc Sp Ex, 51, 4, 630-639).
Dry Needling
Dry Needling has been shown to result in significant improvements of muscular endurance of knee extensors and hip flexion that persisted 4 wk posttreatment as well as a short-term improvement of muscular endurance of knee flexors in the intragroup analysis of soccer players. Compared with placebo, DN showed a significant effect on hip flexion that persisted 4 wk posttreatment. Compared with a nontreatment control, DN also significantly improved maximum force of knee extensors also 4 wk posttreatment. Compared with a nontreatment control, placebo laser combined with water pressure massage resulted in a small but statistically significant improvement of hip flexion range of motion at treatment end and 4 wk posttreatment (Haser et al 2017 Medicine & Science in Sports & Exercise . 49(2):378-383)... further information...
Foot pronation and knee valgus
The arch of the foot comprises several bones. One of the main joints in the arch is the talo-navicular joint which is a 'ball & socket' joint, meaning that it is designed to allow a lot of rotational movement. The talus sits under the tibia (shin bone) and hence influences it's movement.
Tibial rotation is accompanied ankle inversion/eversion and mid foot inversion/eversion
Combinations of shoes and orthotics can greatly influence the tibial rotation.
Anterior cruciate ligament (ACL) and the menstrual cycle
Women are 2-8 times more likely to rupture their ACL than men, suggesting a hormonal mechanism behind this observation (Konopka et al DOI:10.1177/0363546516646374). The ACL is designed to prevent forward shearing of the shin bone (tibia) on the thigh bone (femur). Anterior knee laxity (AKL) and hyperextension of the knees were shown to be significant predictors of anterior tibial translation (ATT) in both males and females. Interestingly the restraining structures to knee hyperextension are the posterior cruciate ligament (PCL) and popliteus muscle, suggesting that the knee in non weight bearing is in a relative posterior position and hence allows for greater total anterior excursion of the tibia. Notably, if a females AKL changes as much as 3mm across her menstrual cycle the ATT changes by 2mm which represented a change of approx 30% in mean magnitude of the ATT (Schultz et al 2011 Med Sc Sp Ex, 43, 2, 287-295). Furthermore, in another investigation, the same authors demonstrated increased absolute and relative magnitudes of multiplanar knee laxity changes. These were seen as increased valgus coupled with relatively greater external rotation of the tibia, making the knee more susceptible to injury on ground contact and early in the landing phase (Schultz et al 2012 Med Sc Sp Ex, 44, 5, 900-909)
Women on the contracetive pill and ACL injuries
Researchers looking at US insurance claims between 20007 and 2017 found that women on the pill were less likely to have an ACL injury whilst playing sport. Reconstructive knee surgery was performed on 569 out of 82874 women who were not on the pill versus 465 out of 82874. Thus the synthetic oestrogen and progesterone hormone were considered protective against knee injuries (De Froda et al 2019,The Physician and Sports Medicine, April)
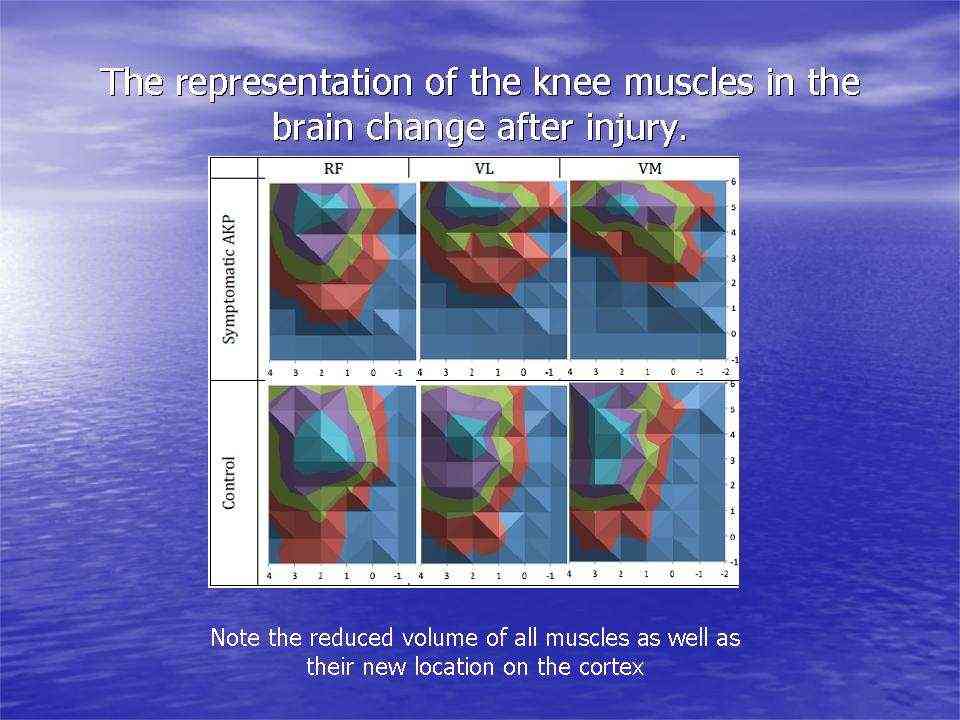
Muscle activation around the knee after injury affects cortical representation of muscles in the brain
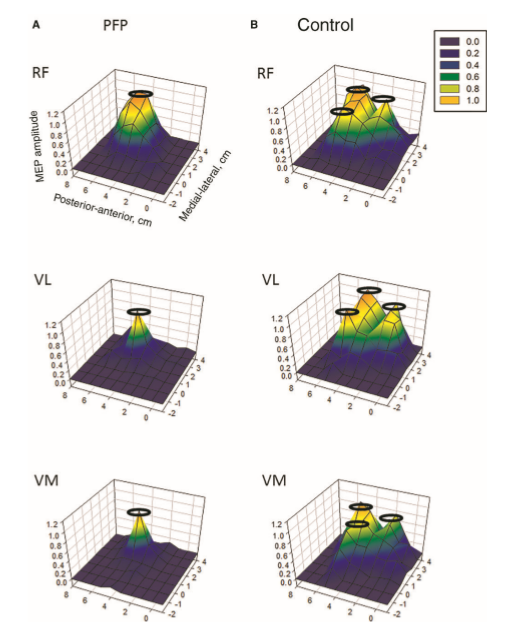
Cortical representation in Patellofemoral Pain (PFP). Note the loss of topography. Te et al (2017) Pain Medicine, 0, 1-11
Transcortical muscle stimulation imaging (Abrahao Fontes Baptista 2014)
Activation of Vastus Medialis and Vastus Lateralis in females with Patellofemoral Pain
Imbalances between the quadricep muscles on the inside and outside of the knee cap have been used clinically for many decades to explain knee pain at the front of the knee, a.k.a anterior knee pain or patellofemoral pain (PFP). Investigators using high density surface EMG of the Vastus Medialis (VM) and Vastus Lateralis (VL) have shown 2 different types of PFP in a group of 36 females. One clinical presentation is that of weaker knee extensor (quadriceps) strength but more subtle fine tuning between the two muscles with a tendency of VMO to work preferentially during eccentric (muscle lengthening) contractions, whilst VL worked preferentially during concentric (muscle shortening) contraction. Whereas the other presentation was the inverse where stronger knee extensor (quadriceps) strength was accompanied by less differentiated VM : VL task specific function (Gallina et al 2018 Med Sc Sp Ex, 51, 3, 411-420).
Muscle activation around the patella and the menstrual cycle
The initial firing rate is lower in the VMO (vastus medialis oblique) compared with VM (vastus medialis) in women not men. The firing rate is affected by the menstrual cycle, showing increases in initial firing during the early follicular phase through tp the late luteal phase. The initial firing was lower in VMO compared to VM during ovulatory and midluteal phases (Tenan et al 2013, Ex Sc Sp Ex, 45, 11, 2151-2157). This could play a bearing on anterior knee pain due to an increased lateral gliding of the patella over the femur, leading to patellofemoral syndrome.

Fatigue, gait and neuromuscular asymmetries after acute ACL rupture
Patients have been shown to have reduced peak knee moments for both flexion and extension in the injured knee. However, the size of the reduction in extensor moment was greater than reductions in flexor moment, when compared between limbs (Gardinier et al 2012, Med Sc Sp Ex, 44, 8, 1490-1496).
A series of squats, bilateral height jumping, and single limb landing exercises were used to induce fatigue in a population of post surgical ACL repaired males. Interestingly, altered joint biomechanics was seen, even at moderate levels of fatigue (<50%). Interestingly, little inter-limb variation was see, except for a reduction in hip extensor moment, which may represent a compensatory strategy to reduce the demand on the knee when jumping from a height. Both knees landed in more abduction (outward positioning) as fatigue set in (Webster et al 2011, Med Sc Sp Ex, 44, 5, 910-916).
Neuromuscular function during a forward lunge in meniscectomized patients
Researchers have demonstrated increased muscle coactivation, reduced range of motion, and increased rate of loading in the operated limb when compared to the other side (Thorlund et al 2012, Med Sc Sp Ex, 44, 7, 1358-1365). This coactivation was mainly the result of increased hamstring muscle activity. Another, investigation by the same researchers, during stair descending demonstrated reduced medial versus lateral muscular activity in the operated leg (Thorlund et al 2011, Med Sc Sp Ex, 43, 7, 1272 - 1279). In a 2 year longitudinal study, post medial meniscectomy, it was shown that those subjects who underwent surgery had greater eccentric muscle strength deficit (8% and 9% hamstrings and quadriceps resp) as well as increased external knee adduction moment. The reduction in these mitigating factors are considered significant in that they may be a contributing factors to the early onset of osteoarthritis (Hall et al 2013, Med Sc Sp Ex, 45, 11, 2036-2043).
Stages of injury
Mental health among athletes is an important consideration that has recently gained more attention. The 2019 International Olympic Committee (IOC) consensus statement on mental health in athletes reported on the high prevalence rate of mental health symptoms in athletes and the relationship of mental health with physical injury and subsequent recovery (Reardon CL et al 2019 Br J Sports Med. 53, 11, 667–699). The IOC urged that mental health is a vital component of athlete well-being and cannot be separated from physical health. Assessment of mental health and subsequent management should be a routine part of the medical care of athletes. The IOC also concluded that cognitive, emotional, and behavioural responses are important factors in injury outcomes, and mental health disorders can complicate recovery. A systematic review of 28 studies reported 65% of those patients not returning to play cited a psychological reason for not returning (Nwachukwu, BU et al 2019 Orthop J Sports Med. 7, 5, 23259 67119845313). Fear of reinjury, lack of confidence in the knee, and depression were the most commonly cited psychological reasons.
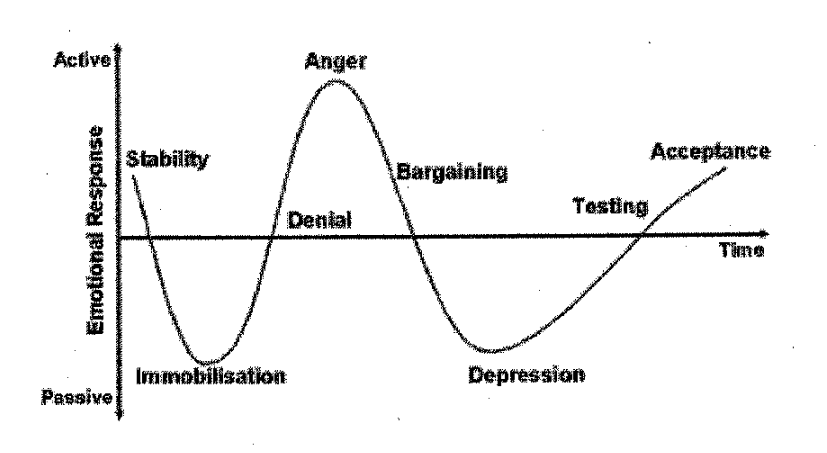
The mental health and the psychological stages of injury and recovery are an evolving continuum.
-
Denial
Athletes begin an internal dialogue trying to convince themselves that it's not that bad. They try to get up and run or jump or convince themselves that it will be better in a couple of days. In extreme cases, athletes pretend there is no injury.
-
Anger
"Why me?" or "Why now?"
-
Bargaining
Athletes accept the injury and endure the pain, but they try to ignore it or overcome it by adapting their training to avoid the injured area. Generally performance drops and compensatory strategies create imbalance and over loading of other structures or body parts.
-
Depression
If your training and goals were well planned out, your injury can have a greater impact, because it's more obvious what's missing. Hormonal considerations such as the lack of endorphines from training also play a critical role.
-
Acceptance
For rehabilitation to be effective, this is the stage you need to get to. The preceding stages are completely natural and understandable. Recognize them for what they are. You can start working on your rehab right away, even while you are going through the other stages.
Characteristics of an athlete who is psychologically ready to RTS are multifaceted and include, among others: realistic expectations, high levels of self-efficacy and low levels of anxiety (Forsdyke D 2017 https://bjsm.bmj.com/content/51/7/555.full).
Treatment and exercises for knee rehabilitation
Whilst working in Switzerland, with professional soccer players, from the Italian Series A and German Bundesliga, I noted that soccer players have relatively tight hamstrings, adductors and hip flexors, and well developed calf, quadriceps, hamstrings and gluteal muscles. Investigations have demonstrated that localised application of vibration can improve passive knee extension in women (Bakhtiary et al 2011, AJP, 57, 165-171). Studies have shown that women's hip muscles can atrophy after an injury as simple as an ankle sprain, due primarily to injury-caused limping or using crutches. Any hip or core muscle weakness, when combined with a woman's biomechanics, can be detrimental to a female athlete returning to the soccer field. Proper rehabilitation is critical to coming back from an injury stronger and healthier. From the previous discussion, it would appear that neuromuscular balance and control are exceedingly important factors in the rehabilitation of the knee. Moreover, hip-back-pelvic-foot dynamic control are critical for a return to function and sport.
Resolution of knee impairments, including range of motion and effusion, and strength and hop testing are supported by the literature, and newer studies of movement symmetry are actively being studied. A positive correlation has been reported between isokinetic knee extension peak torque and subjective knee scores as well as 3 hop tests (Wilk et al 1994, J Orthop Sports Phys Ther 20, 2, 60-73). Also, a good positive correlation was reported between knee extension acceleration rate and deceleration range for a timed hop test and triple crossover hop. Quadriceps strength deficits may be associated with increased risk of reinjury. One study reported that 33% of patients with quadriceps strength <90% of the contralateral extremity suffered reinjury as compared with 13% of those with >90% quadriceps strength symmetry (Grindem, H 2016 Br J Sports Med, 50, 13, 804-808).
At the Rhennbahn Klinik (1992-3), under Dr Bernard Seggesser, we found isokinetic quadriceps assessment (esp 0-40 degree ROM), stabilometry and hop testing particularly useful amongst professional soccer players. We also used a sports field opposite the Klink, to test sports specific functional outcomes.

Meniscal injuries with ACL injury
An investigation by the Rennbahn Klinik, comparing isokinetic strength, 6 months post op, ACL vs ACL and Meniscal Repair, demonstrated strength deficits, particularly when the lateral meniscus was involved (Wenning et al 2020 Arch Orthop Trauma Surg 40 6, 751-760). Six months postoperatively overall there is no significant difference between the groups (extension strength MR 82% vs. CON 85% and flexion strength 86% vs. 88%, resp.). Subgroup analysis showed that medial repairs exhibit a comparable leg symmetry while lateral repairs performed worse with leg symmetry being 76% in extension and 81% in flexion strength. Patients undergoing BM repair performed in between lateral and medial repairs (82% extension, 86% flexion). However, this is still short of the 90% strength deficit minimum recommended for RTS. One study reported that 33% of patients with quadriceps strength <90% of the contralateral extremity suffered reinjury as compared with 13% of those with >90% quadriceps strength symmetry (Grindhem H et al 2018 Orthop J Sports Med, 6, 5, 23259; Grindem H, et al 2016 Br J Sports Med 50 13 804–808). .
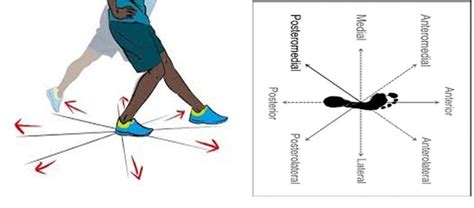
Evasive side stepping
It has been demonstrated that evasive side stepping during sport, against an opponent, activates different postures and knee moments (Lee et al 2013, Med Sc Sp Ex,45, 9, 1740-1748). Hence, stimuli realism needs to be incorporated into ACL rehabilitation programs in order to activate visual-perceptual-motor skill complexity that is required during side stepping.
Medial - Lateral Knee Stability
Engagement of the hamstrings to extend the knee
Core Stability for Knee Stability
Hip Stabilisation for Core and Knee Stability
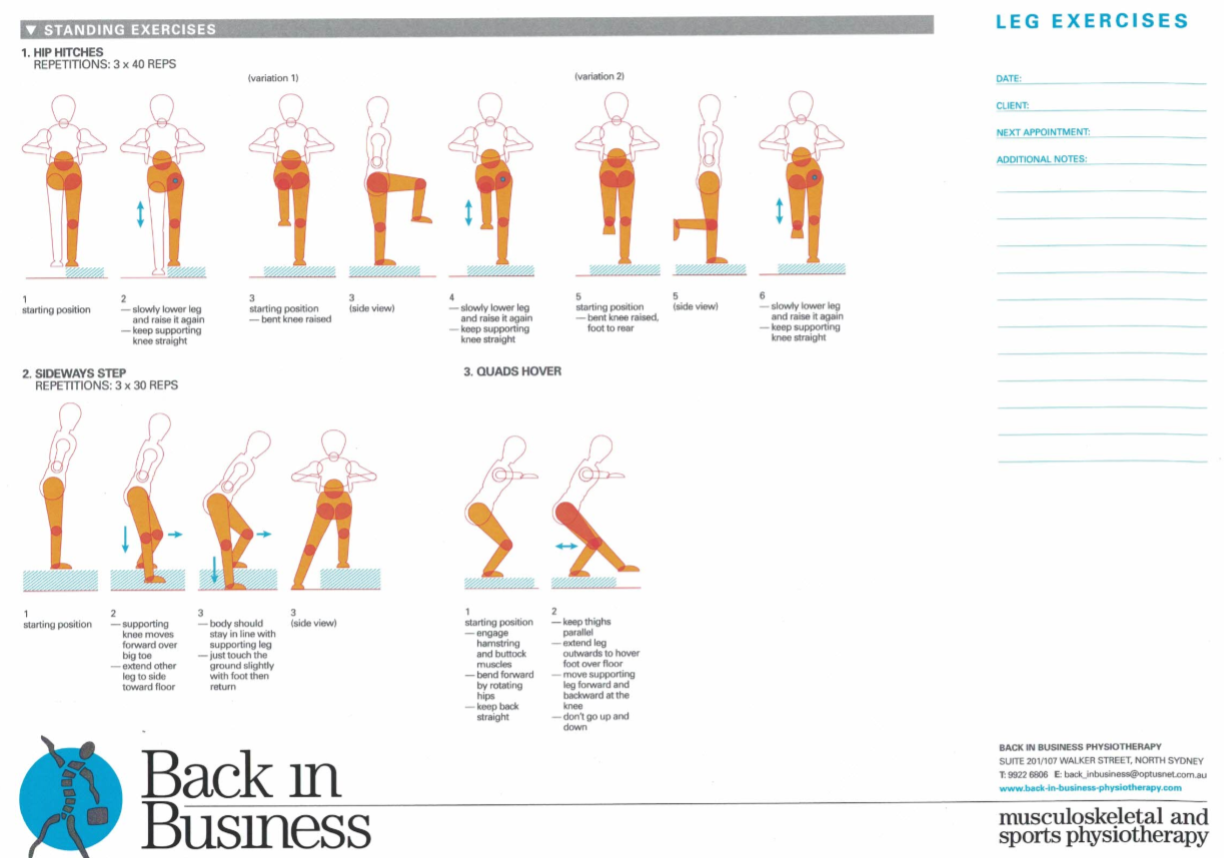
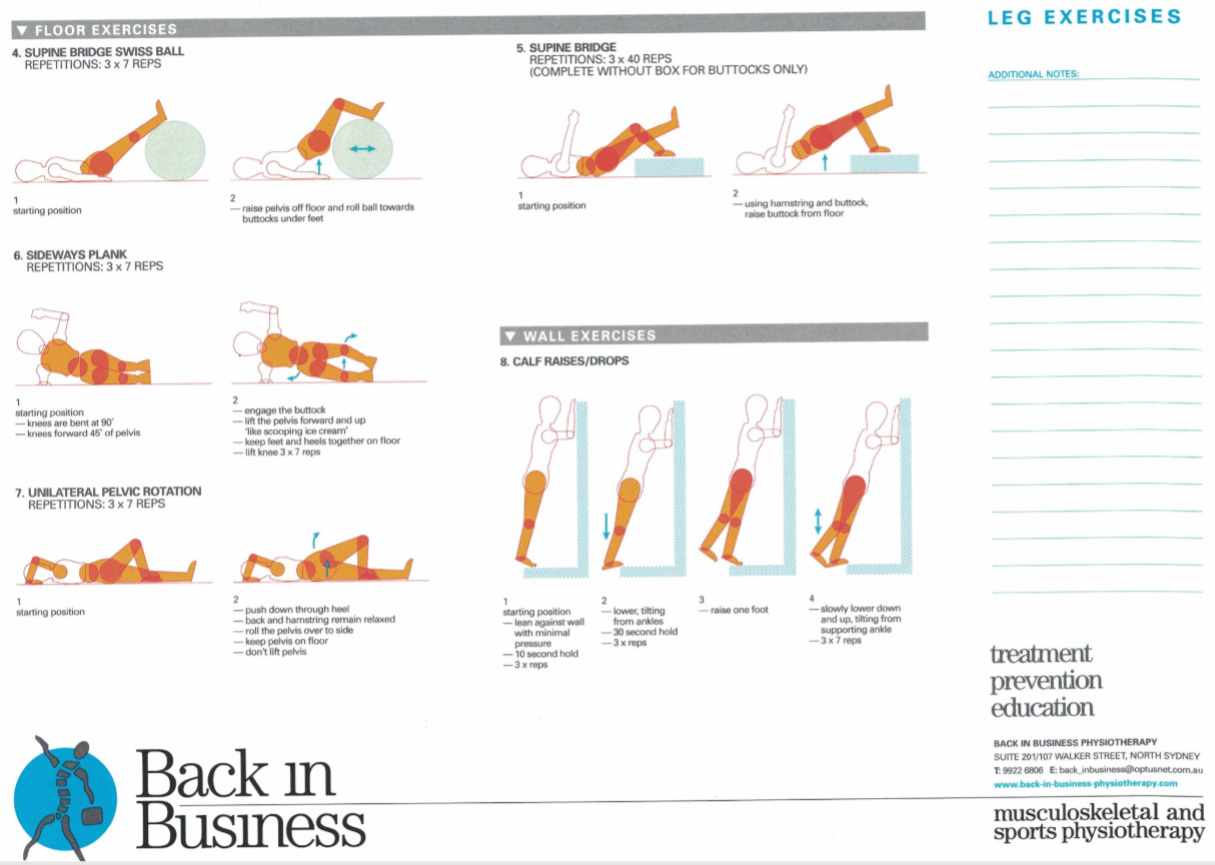
On field rehabilitation should include
- forward - backward running
- sideways running - foot to foot, foot over foot
- running in ever smaller circles
- figure of 8 running
- running with ball and doing tricks with ball
- soccer drills
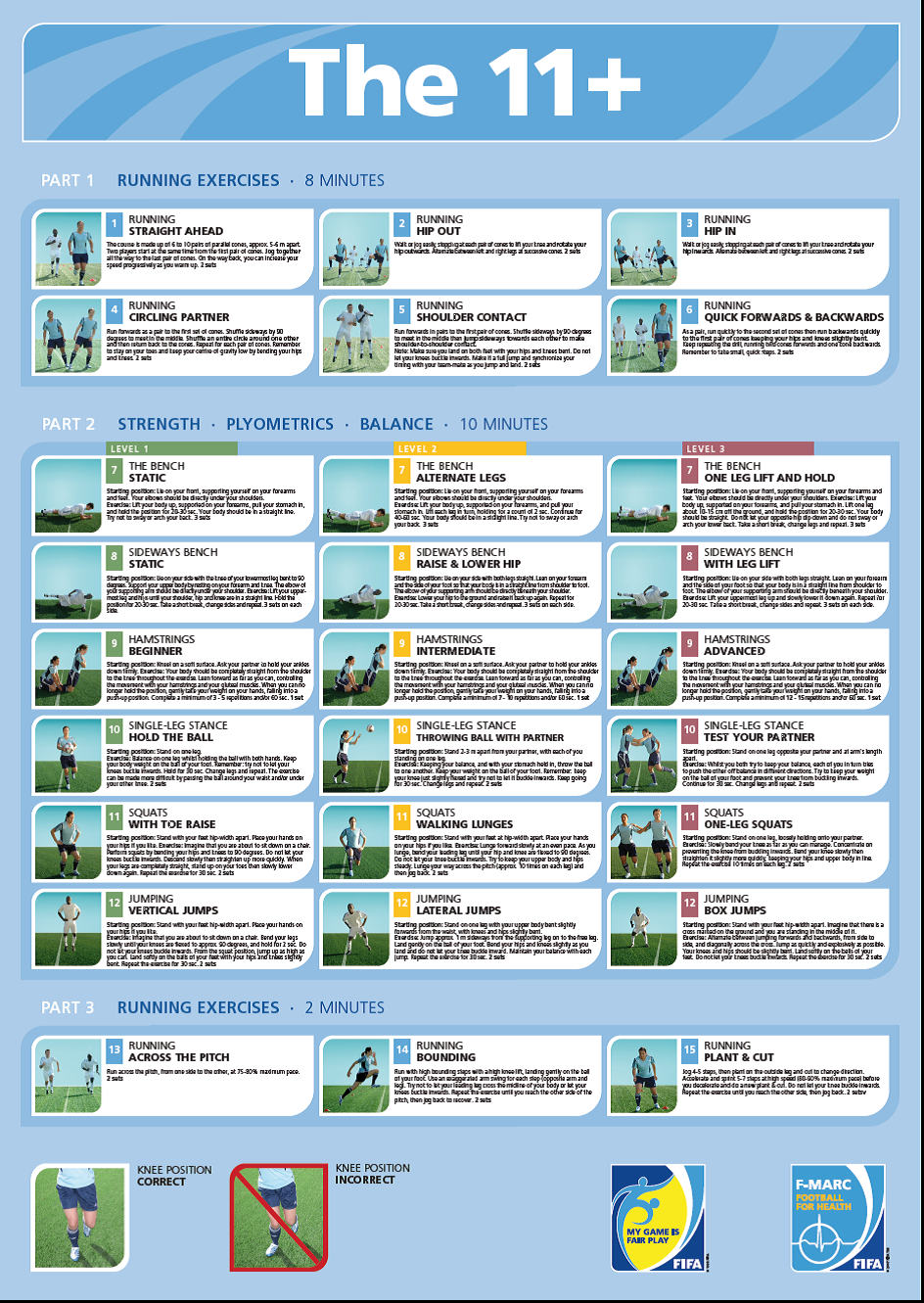
- FIFA 11 Plus
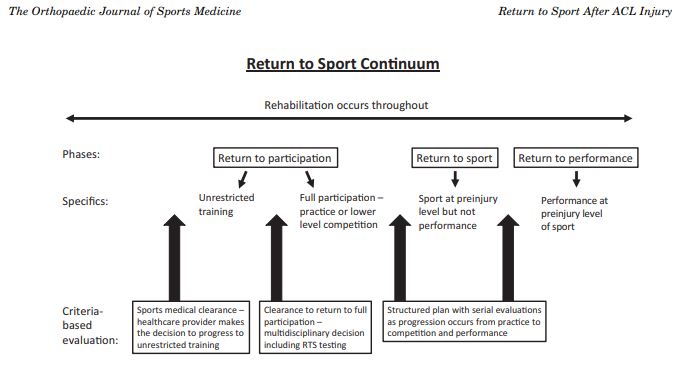
Consensus return to sport (2020)
A systematic review reported that greater quadriceps strength and less effusion were the physical examination findings associated with successful RTS.(Czuppon S, et al 2014, Br J Sports Med. 48, 5, 356–364). It has also been reported that hamstring-to-quadriceps strength ratio deficits and failing to pass a clinical test, involving quadriceps strength and single-leg jump testing, were associated with higher ACL graft rupture rates.(Kyritsis P, et al 2016 Br J Sports Med. 50, 15, 946–951). Additionally, for every 1% increase in quadriceps limb symmetry index, there was a 3% reduction in subsequent knee injury risk.(Grindem H et al (2016) Br J Sports Med. 50, 13, 804–808). The objective physical examination should be conducted with the understanding of the patient’s individual sport, where some measures may be more relevant. Although the physical examination may be considered the baseline assessment for monitoring knee injury recovery, multiple other criteria, such as RTS functional testing and psychological assessment, should also be met before RTS.
Link to PDF on Delphi Consensus on RTS
RTS testing should involve assessment of specific functional skills that demonstrate appropriate quality of movement, strength, range of motion, balance, and neuromuscular control of the lower extremity and body. The most commonly reported functional tests are jump tests, including single-leg jump, crossover jump, triple jump, and timed jump tests typically comparing with the contralateral limb.1 Quadriceps and hamstring strength testing have also been extensively reported, and agility testing and motion analysis are reported commonly as well. Star excursion balance testing has been shown to be a noncontact lower extremity injury predictor, and ACL reconstruction patients have been reported to have residual deficits on these tests when returning to play (Butler et al 2013 Sports Health 5, 5, 417–422; Clagg et al 2015 J Orthop Sports Phys Ther, 45, 6, 444-452) In addition, drop vertical jump testing and postural stability tests were reported to predict higher reinjury risk after ACL reconstruction in young athletes. (Paterno MV et al 2010 Am J Sports Med. 38, 10 1968–1978).
The RTS continuum emphasizes a carefully structured stepwise progression of return to practice first and then return to competition. Clearance to full participation (practice followed by
competition) should be a multidisciplinary decision involving the patient, parent if the patient is under 18 years of age, surgeon, team physician, and physical therapist/athletic trainer (agree 26/26; 100%). RTS occurs along a continuum, and there is a shared decision-making process that occurs over time and with multiple contributors. There are different medical and technical competencies between the different contributors (surgeon, team physician, physical therapist/athletic trainer) in this process. The principles of shared decision making apply, and the patient is actively involved. A multidisciplinary decision must be made with reasonable compromise from all groups if dissent exists. This multidisciplinary approach requires well-defined roles, communication among all parties, and a system to protect the athlete from disparate risk tolerances.
The decision of clearance to unrestricted training is multifactorial and should consider the time since injury, treatment, clinical examination, RTS testing, psychological readiness, and sport-specific conditions. Competing interests and expectations of those involved in the RTS process (eg, patient, family, coach, club, surgeon, team physician, physical therapist/athletic trainer) should be recognized. Ultimately, the decision to provide clearance to begin progressing the patient’s training is to be made by the health care provider, including physician or physical therapist/athletic trainer. This is an important distinction determining that the health care provider alone should make this initial decision to progress to unrestricted training. With any conflict of interest, the health care provider’s ethical obligation is to the patient’s health. Although the team physician may experience conflicting pressures, they must be transparent and inform the patient about any concerns so that the patient is adequately informed. These contextual factors make the clearance decision demanding and emphasize the importance of understanding the RTS process as a continuum with a criteria-based stepwise approach.
Inclusion of the coach as a decision-maker in this consensus statement did not reach consensus (7/26; 27% agreement). There was concern that inclusion of the coach in the medical decision would create a conflict of interest, given the coach’s obligation or commitment to the team. The primary obligation of the health care provider is the patient’s health, whereas the coach remains focused on the success of the team (Flint, FA and Weiss, MR. 1992 Can J Sport Sci. 17, 1, 34–40). Nevertheless, the coach, as a key person in the sport development of the athlete, needs to be informed and involved in information sharing as the athlete progresses toward sports participation.
How should a club, manager and a team deal with a player who has suffered an ACL injury
The Liverpool 2021/1 EPL season was a classic example of what can happen when a key player suffers an ACL injury. In this case it was Vigil Van Dijke, who suffered an ACL injury from a tackle by England's No1 goal keeper Jordan Pickford. The remaining season was a struggle for Liverpool. In the 2021/2 season, Liverpool started very strong, with the playmaker Virgil, not only defending well, but creating the build up for the offensive play. See video for more details : https://youtu.be/NzfutZBfivM
7 November 2021
 What We do
What We do What We Treat
What We Treat



















































































































