



Mechanical Traction (of the low back and thorax), possible mechanisms and the Musculoskeletal Physiotherapeutic assessment of signs and symptoms to ascertain effective dose
Martin Krause (1995, 1999, 2004, 2006, 2020) M.Appl.Sc (Manip Physio), Grad.Dip.Hlth.Sc (Sport & Ex), Grad.Cert.Hlth.Sc.Edu, Cert IV Workplace Assessment & Training
Myths : "mechanical traction acts on the 'bulging' intervertebral disc which is impinging on the sciatic nerve"
despite
- 48-52% of the asymptomatic population having a disc hernia on MRI imaging
- peri-radicular injections being able to improve the clinical signs and symptoms of 'sciatica and disc hernia'
- the intervertebral foramen, and it's contents, consists of more than just the disc. In fact it is made up of bone, zygapophyseal joint, ligaments, Batson's venous plexus, pia mater, dura mater, sinuvertebral nerve (SNV), spinal nerve, nerve root and dorsal root ganglion
- neurophysiology of pain and inflammation processing, immune physiology and 'deterministic chaos' suggesting that any disruption of continued ectopic input generation could normalise neurological signs and symptoms.
Synopsis
The following describes a 'two threshold' dose methodology, for the use of mechanical traction, in the treatment of low back pain, in particular radiculopathy. A rational is presented using both clinical phenomenon, as well as face and construct validity, from the realms of clinical reasoning, biomechanics, neurophysiology and immunology. The bulk of work was undertaken in 1995 as a Masters Treatise. Revisions were made for a key note presentation at IFOMT (International Federation of Manual Therapy) at the WCPT (World Confederation of Physical Therapy), in Yokohama, Japan, in 1999. The slides presented here are those original slides! Further presentations were made at conferences and workshops in Chile and Brazil. The original work was accepted for publication by the Journal of Manual Therapy in 2000. Further reviews were undertaken, by me, in 2004, 2008 and 2020. I hope the clinician/reader finds the discussion stimulating and enlightening. The evolution of thinking and paradigm shifts, from a high loading mechanical 'passive' rationale to a low loading immune neurophysiologically interactive rationale are highlighted. Importantly, a paradigm shift was proposed whereby, pathology of the poorly innervated intervertebral disc (IVD), is considered as a spectrum of an inert mass of tissue pressing against a nerve, to an inflammatory - immune model involving the highly innervated contents and structures comprising the intervertebral foramen (IVD) and spinal canal. As such a 'two threshold' hypothesis for dose was developed, whereby the initial low threshold of 'normalisation' of signs and symptoms (S+S) represented 'unloading' of the blood vessels and contents of the IVF, whereas the second threshold of deterioration of S+S represented 'overloading' of the IVD and/or posterior longitudinal ligament (PLL) - Batson's venous plexus. The two threshold dose hypothesis, in a range between 7 and 25kg, requires further verification, in particular the identification of which populations would benefit most from such an intervention. The next step, on the path to the evolution of thinking, will be the involvement of deterministic chaos, which can be read elsewhere on this site.
Table of Contents
Dorsal Root Ganglion (DRG)
Conditioned & Unconditioned Stimuli
Modulation of Mechanoceptor Activity
The Locus Coeruleus response to treatment stress
The role of feedback to descending modulation of pain and inflammation
Impaired Brain Processing w.r.t emotions and catastrophising
Theoretical Explanations - original paper on the effect of mechanical traction on neurogenic inflammation (1995)
Sensory Discriminative - Motivational Affective Components of Pain Processing
Ectopic Impulse Generation by the DRG
Normalisation of Signs and Symptoms using Traction
Clinical Implication of Neurophysiology on a 'Two Threshold' hypothesis
Validity of using the normalisation of signs and symptoms to establish the dose
Neurogenic inflammation and the cytokine immune response
Reduction of Venous Congestion
Sinuvertebral Nerve and Sympathetic Somatic coupling for healing
Introduction
The brain's neural processing has been likened to a symphony orchestra playing in tune (Goldstein JA 2004). A type of resonance termed 'neural synchronicity' has been related to arousal, attention selection, and working memory. Grossberg (2000) highlights the relationship between matching top-down expectations with bottom-up data, a process which focuses attention on those features of the bottom-up input that are expected. The interaction of attention-learning and orienting-search subsystems and how they interact has been developed into adaptive resonance theory (ART). If there is appropriate stimulus generalisation then amplified representation can, in turn, attentionally block or inhibit the representations of irrelevant sensory events (Goldstein JA 2004). It is proposed that, radicular pain may represent a disturbance to CNS data processing and appropriate treatment may represent the attention block which can inhibit unwanted signal 'noise' help re-establish neural synchronicity or fidelity to the system. Perhaps a differentiation should be made between acute and chronic pain, whereby, in the acute scenario this 'fidelity' requires removal of unwanted noise, whereas in the chronic scenario, the aberrant 'normal' input is the outlier required for a deterministic chaos hypothesis to be applied to the mechanisms behind the effect of manual therapy and mechanical traction, in particular. Either hypothesis would suggest that purely assessing neurological signs and symptoms, during the selection of the appropriate dose of treatment, could employ 'fidelity normalisation' through the mechanical removal of irritant input, such as oedema and/or inflammation, whilst the sensory perception of 'normalisation' applies the reference point needed 'to jump' to that normalised state. This 'jump' being a neuro-inflammatory-immunological response. (in depth analysis of deterministic chaos can be found : Krause M 2020 https://www.back-in-business-physiotherapy.com/health-advocacy/exercise-and-the-immune-system-during-covid-19.html)
Beginning of slide presentation
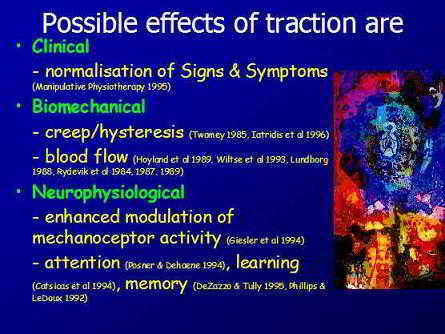
Generally, indications for the use of traction are for people suffering from a spectrum of low back pain (LBP) with leg pain, pins and needles, numbness, loss of muscle power, and who are classically assigned to a diagnosis of a pinched nerve, slipped disc, radiculopathy, nerve root irritation or sciatica, would be considered as candidates for treatment with mechanical traction. Traction has been used since the times of ancient Greece. Some of the beneficial effects of traction include the immediate normalisation of S+S, including neurological ones.

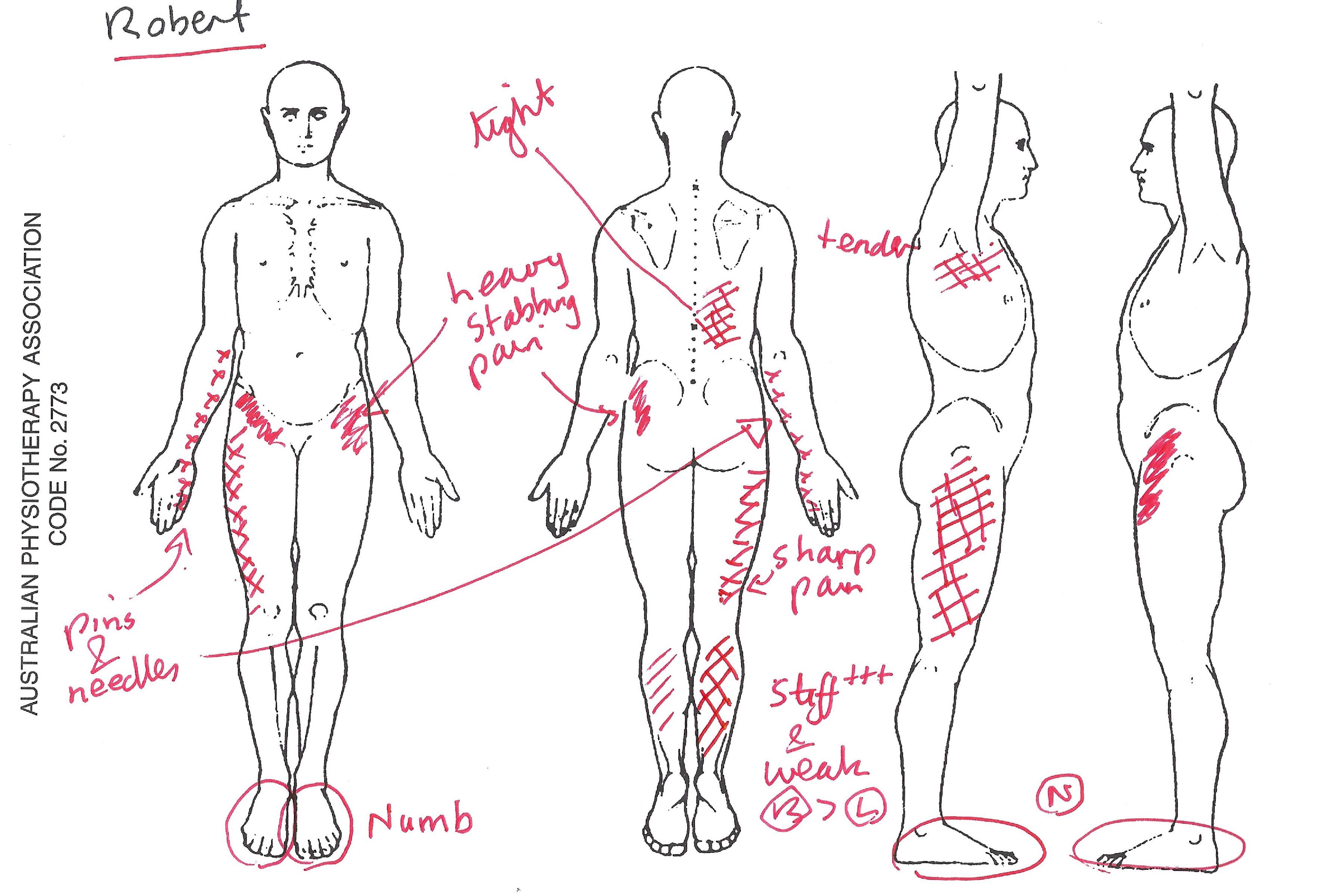
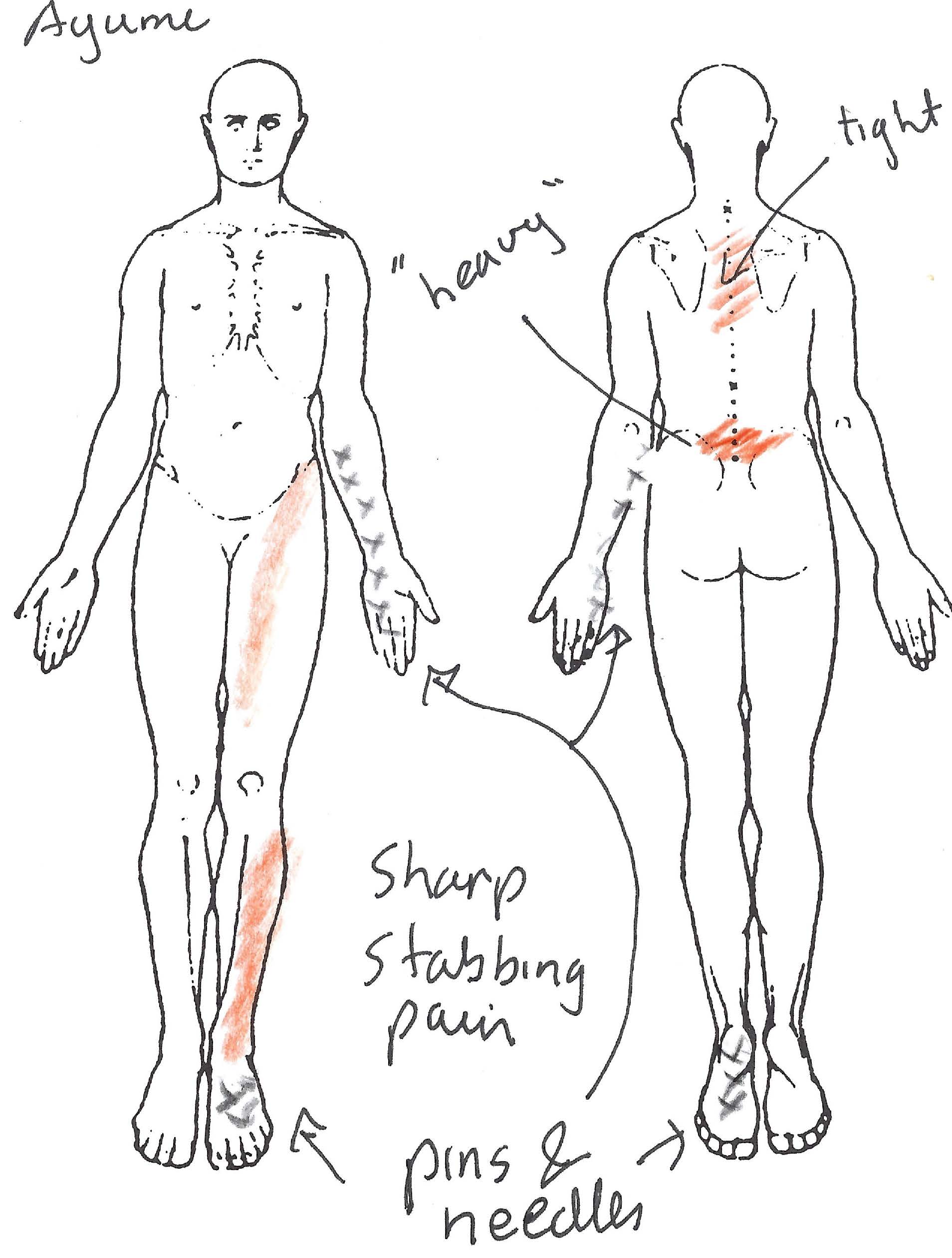
Clinical presentation - leg pain referral patterns from lumbar spine irritation
Typically, LBP which is accompanied by a leg pain distribution pattern, as demonstrated by the work by Nikolai Bogduk (1980), would be a clinical picture where treatment with mechanical traction would be considered.
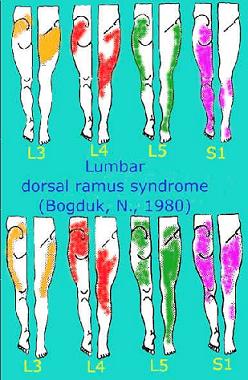
Interestingly, these referral patterns represent somatic structures of the dorsal spine. Irritation of the Spinal nerve and Dorsal Root Ganglion (DRG) in the Intervertebral Foramen (IVF) have similar referral patterns, but generally include neurological signs and symptoms such as loss of sensation, altered tendon reflexes and reduced muscle power.
Motorised Mechanical Traction

There are several different types of mechanical traction. The one considered here is 'motorised traction' which has some similarity to the principles of auto-traction and passive traction. Here, an opening and sliding bed is used to provide a friction free table. Suggestions have been made, that this allows the use of smaller doses, as the bed gaps at the level of the spine where distraction is supposed to take place. Patients are traditionally lying on their backs, with their legs up at 90 degrees, or straight with a roll under the knees for approximately 30 degrees flexion. Other 'non-traditional positions' have been used, such as 'the position of comfort' which frequently resembles the (only) way the person can sleep at night. These conditions tend to severely affect peoples ability to sleep, where, out of desperation, they become very inventive in what position attains most relief. Other positions used may resemble a directional preference for 'unloading' or 'loading' certain spinal tissue, depending on the stage, stability, irritability and severity of the condition.
Indications
Indications for the use of traction, include people suffering low back pain, with either leg pain and/or pins & needles or numbness. Altered tendon reflexes and loss of muscle power may also be present.

The above two positions show 'non-traditional' positioning for the application of lumbar mechanical traction. Although the scientific evidence for mechanical traction is poor, the above positioning, demonstrates the inventiveness of clinicians and how the clinical process rarely conforms to the rigidity of reductionist scientific endeavour and the 'one shoe fits all' scenarios needed for comparing supposedly heterogeneous populations. Frequently, when it comes to radiculopathies, the client presents with an antalgic posture such as a pelvic shift or list. This position of comfort can be used in the acute phase of treatment with traction.
Normalisation of signs and symptoms
Clinically, a two threshold hypothesis, has been used, by Australian Manipulative Physiotherapists, to select dose. The first threshold is that where neurological signs & symptoms (S+S) normalise, whereas the second threshold is where it deteriorates once again. These S+S include Achilles and Patella tendon reflexes, muscle power, skin sensation and Neural Tension Signs such as Prone Knee Bend (PKB) and Straight Leg raise (SLR). The second threshold may represent considerable strain on a hypermobile or damaged intervertebral segment, whereas the the normalisation 'window' represents unloading of the Intervertebral foramen (IVF) contents. Additionally, pure reliance on body weight ignores client morphology, including hypermobile people (Ehler Danlos Syndrome and JHS), their age, physical fitness/resilience, etc.
Investigators (Meszaros et al 2000, JOSPT, 30, 10, 595-601) demonstrated improvements in SLR at various doses of traction. They compared the effect of 10%, 30% and 60% body weight in 10 people (9 males and 1 female), weighing 61.2kg -> 118.8kg, ages ranging from 17 -> 55 years. They found improvements in SLR range of movement (ROM) from 24.1º to 27.4º + 13.0º(@10%BW), 34.0º + 14.3º(@30%BW) and 36.5º + 15.8 (@60%BW). There seems to be a wide variability in these results. Furthermore, based on a risk : benefit ratio assessment, is going from 30%BW to 60%BW worth those 2º? It should be noted that all the subjects had at least one additional neurological sign, however the examiners only noted that the application of traction was pain free and didn't report on the result of traction on those additional S+S.
SLR is considered a reliable, although non specific, predictor of disc hernia. Only a small amount of hip flexion is necessary to initiate movement of the spinal nerve in the IVF. It is thought that compression and/or inflammation of the neural tissue sheath can instigate reflexogenic muscle spasms, limiting ROM (see subsequent article below).
It's also been my clinical experience that the ROM in SLR can improve with improvements in tendon reflexes and muscle power and skin sensation, but it may diverge, with the other S+S deteriorating after a given threshold of loading is reached. This may represent a loss of nerve conduction which limits the capacity for protective reflexogenic muscle spasms when loads are too great. Hence, it's important to take into account the other clinical signs and symptoms. Maitland (1986) suggested that the pain level (VAS) should not improve by more than 50%. People have been known to worsen on traction and even require surgery. Therefore, it's critically important to ascertain the severity, stability, irritability and stage of the clients condition before deciding to apply traction. During the application of traction all S+S should be monitored with progressive loading (1-2kg increments from 7->25kg). The dose selected should be the minimum required to obtain a normalisation of S+S.
Special tests include the neurological assessment and the effect of various positions on those neurological S+S. The subjective examination should create a 'predictive reasoning' approach to the objective - physical examination and those later findings are used to confirm or negate the 'working hypothesis'.
Evidence


Amazingly, a decade after the realisation that the immediate normalisation of neurological signs and symptoms can occur, if the appropriate dose of traction is applied, the research evidence (see Cochrane report (2006) still didn't justify it's use. This, despite it's common therapeutic use for the treatment of acute radiculopathy.
A randomized double blind trial was performed, where 17 subjects with acute lumbar sciatica secondary to disc herniation were assigned to high-force traction at 50% body weight (BW; LT50, n = 8) or low force traction at 10% BW (LT10, n = 9) for 10 sessions in 2 weeks. Radicular pain (visual analogue scale [VAS]), lumbo-pelvic-hip complex motion (finger-to-toe test), lumbar-spine mobility (Schöber-Macrae test), nerve root compression (straight-leg-raising test), disability (EIFEL score), drug consumption, and overall evaluation of each patient were measured at days 0, 7, 14, and 28. Patients with acute lumbar sciatica secondary to disc herniation who received 2 weeks of lumbar traction reported reduced radicular pain and functional impairment and improved well-being regardless of the traction force group to which they were assigned. The effects of the traction treatment were independent of the initial level of medication and appeared to be maintained at the 2-week follow-up (Marie-Eve Isner-Horobeti et al 2016 J Manipulative and physiological therapeutics 39(9)DOI: 10.1016/j.jmpt.2016.09.006)

Entire spinal effect
Researchers used a sophisticated traction device to ascertain traction stiffness and the resulting spinal strain using a finite element stimulation method (Tadano et al 2019, BMC Musculoskeletal Disorders, 20 : 155 DOI: 10.1186/s12891-019-2545-9). Moreover, they recruited, 133 patients with non-specific CLBP, from 28 orthopaedic clinics, to undergo this biomechanical experiment, to assess and determine traction conditions, for subsequent clinical trials.
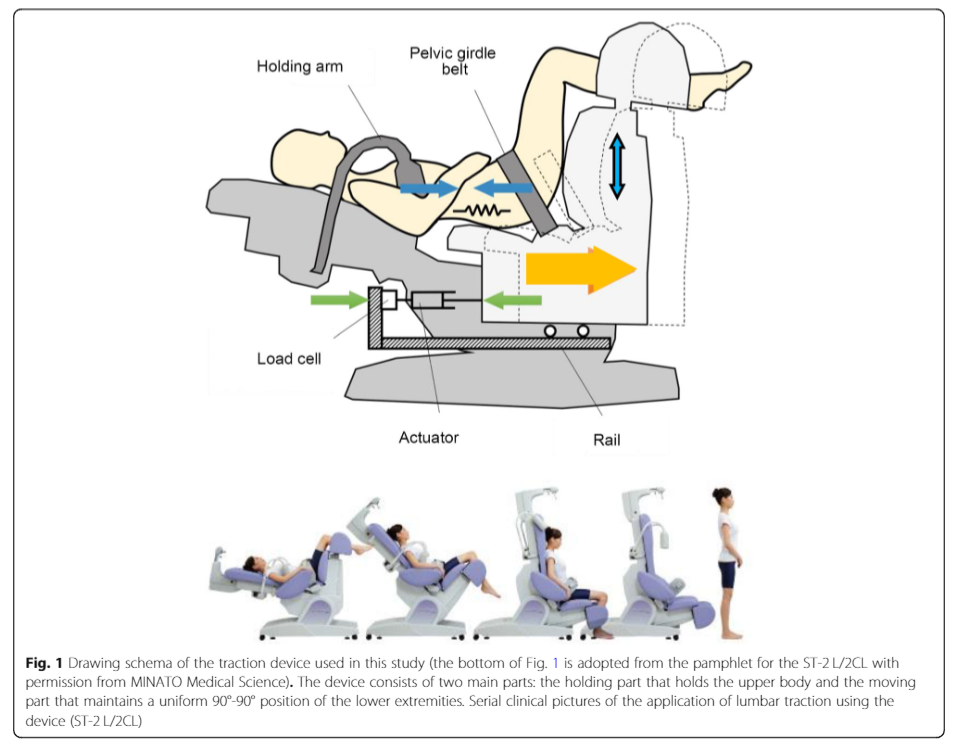
These researchers demonstrated some interesting results when comparing strain, distance and load.
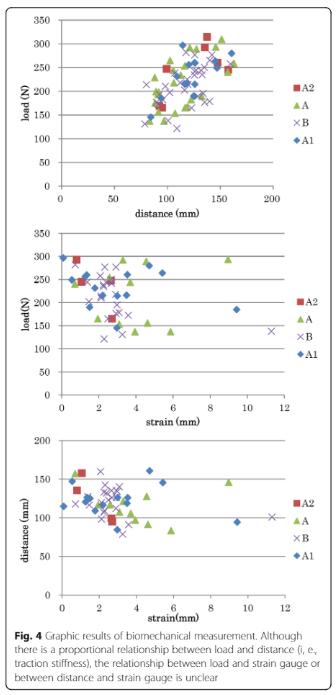
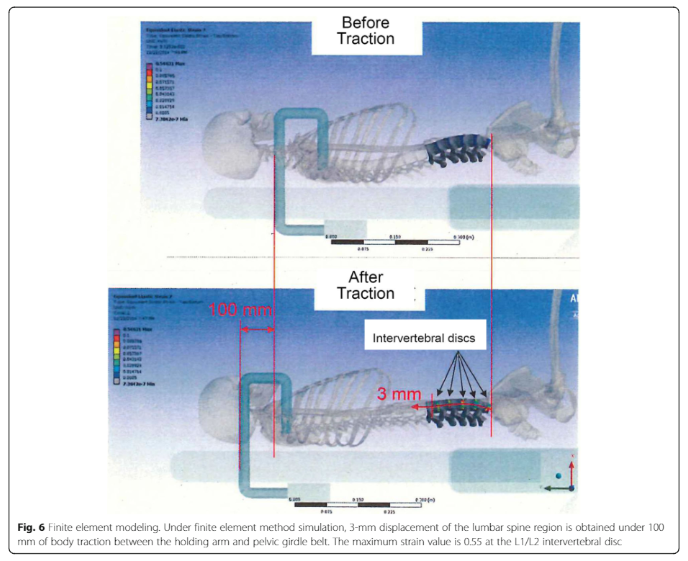
Incredibly, the entire spine was modelled. By doing so, another element of plausible 'mechanism of action', includes the thorax with it's thoracic rings and the sympathetic ganglion chain, residing on the anterior aspect of the dorsal ribs. Moreover, they describe 100mm of body traction required, for a 3mm displacement in the lumbar spine.
Even more interesting, is that these researchers also added a vibration stimulus (40% body weight), to ascertain any further beneficial effects. Please refer to another aspect of this website for Whole Body Vibration. Never-the-less, the vibration would have added another element of mechanoceptive input, as well as potentially stimulated the lumbar multifidus muscles directly and/or indirectly through the localised release of osteocalcin. Additionally, vibration may have effected any oedema or blood flow aspects of the IVF. Finally, vibration may have an effect on the viscoelastic biomechanical elements of the collagen tissue.
Effect of traction beyond the lumbar spine and lower limbs
These Japanese researchers demonstrated an effect of lumbar traction to the thorax. Interestingly, early in 2021 I had a dozen clients with severe LBP, including neurological signs and symptoms. Interestingly, two clients C/O medial (inside) arm 'pins & needles'. So, during the application of traction, using a dose which normalised neurological signs and symptoms, I treated the cervical spine, using Manual Therapy techniques. In these two clients, there was an extra-ordinary reduction in muscle spasm in the cervical spine, from lumbar traction. Taking this further, I was having little progress, in another client, with cervical pain and 'shadowing' in the brain (on MRI imaging). He had a previous history of L3/4 disc problems, some 10 years ago. I applied lumbar traction and again noted significant improvements to cervical and upper thorax mobility. From, February 2021 until May 2021, I applied this methodology on another 48 clients, one of whom had extensive 'arthritis' from Leyden's factor V and Pro Thrombotic Factor gene. This latter client I had treated for years, maintaining her ROM of rotation, flexion and extension, with very little success on improving lateral flexion. From almost no lateral flexion, she gained approximately 3/4 ROM and significantly longer relief between treatment for the other directions of movement. Currently, approximately 2/3 of these 48 clients, have shown dramatic improvements in cervical and arm signs and symptoms, when treatment was carried out in conjunction with lumbar traction. It is highly likely that lumbar traction is affecting the 'thoracic rings', adverse neural tension in the dura mater and mechanical loading of the sympathetic ganglia of the thorax.
Traditional Dose of Traction
The use of high dose mechanical traction was championed by James Cyriax, the father of modern manual medicine, in the 1950's. There are famous photos of two therapists leaning with full body weight, at either end of the patient, for the application of traction. No doubt, four thousand years earlier, the Greeks were using a similar methodology. (Sari H et al 2014 https://pdfs.semanticscholar.org/083a/d13d884a11bb64aafccca0720386b4134787.pdf). This is quite the opposite, to the hypothesis, whereby signs and symptoms, tend to deteriorate at higher doses. Additionally, is it only the disc we're treating or the structures in and around the IVF?

Note the proximity of the intervertebral disc (IVD) to the spinal nerve. Additionally, note the fact that the ventral (front) portion of the IVF is covered by the zygapophyseal joint capsule. Swelling of this joint capsule can presumably add pressure to the contents of the IVF. Such pressure may induce inflammation on these contents, which reduces the threshold of mechanoceptor and nociceptor firing, spinal cord and descending modulation, let alone peripheral sympathetic nervous system and immune modulation. Furthermore, such swelling could alter the mechanoceptor firing with joint movement, leading to altered proprioception, within the capsule, within the Multifidus muscle whose fibrous components blend with the joint capsule. The result of this altered input are muscle spasms and muscle weakness. Presumably, mechanical traction, like soft tissue and joint mobilisations, can be perceived at a mechanoceptive and nociceptive level.
Pain pathology w.r.t. thresholds and tolerances
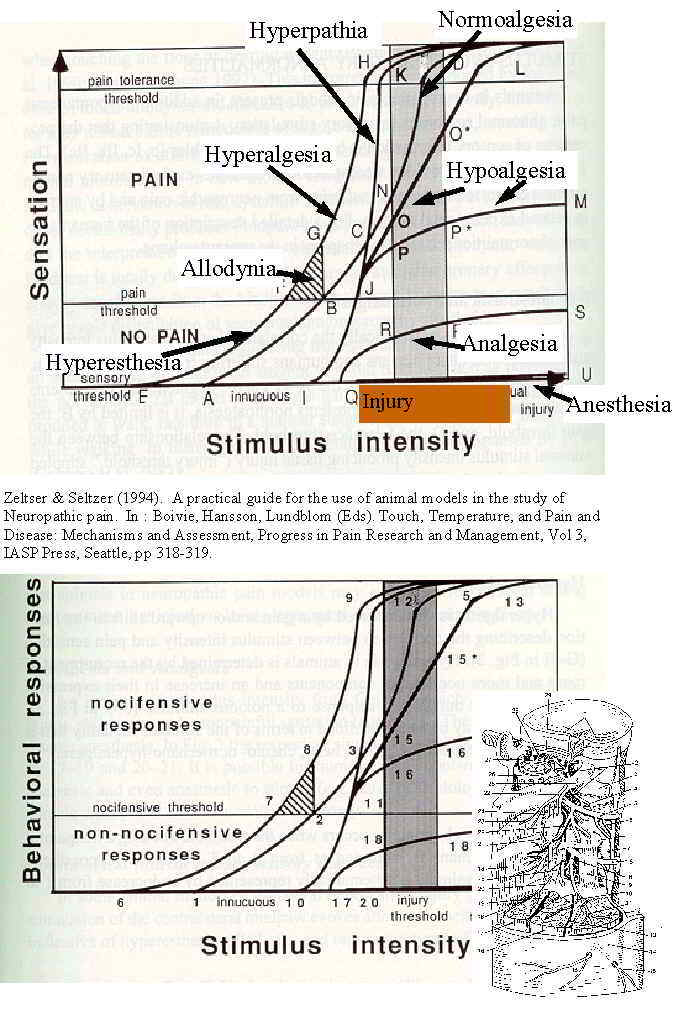
Sorry for the poor quality of the above diagram, however, this is from the first rendition of this website from 1998. The x-axis represents mechanical loading and displacement of soft tissue. Behavioural reactions to this displacement will depend on the 'neuro immune inflammatory state' of the soft tissue mechanoceptors and nociceptors, From the aspect of incremental loading with mechanical traction, there would be a point of unloading the contents of the IVF, which then is followed by a point of loading, where the surrounding tissue of the IVF, is loaded when the distraction becomes too strong.
Joint mobilisations w.r.t. muscle spasms and pain
Clinically, gentle joint mobilisations have been demonstrated to reduce pain and increase ranges of movement, beyond anything which can be explained, by simple biomechanical concepts. of soft tissue creep or hysteresis. So, presumably, gentle spinal mechanical traction can demonstrate similar effects, as it is just another form of joint mobilisation.

An example of the resistance felt when applying pressure to a joint, whilst respecting pain and muscle spasms. The resistance felt from soft tissue and collagen stretching is different to the quality of resistance from muscle spams. In people with functional instability, increased neutral zone or joint hypermobility syndrome, muscle spasms may be the protective background agent preventing harm, where the correct application of muscle spasm reduction requires simultaneous normalisation of postural stabilising muscle tone.
Dorsal Root Ganglion (DRG)
Physiotherapists frequently refer to 'nerve root compromise'. This is a misnomer, as the nerve root sits well within the spinal canal. If the 'nerve root' is compromised this is a serious condition, referred to as cauda equina compromise and requires immediate surgery as bladder and bowel function can be disturbed. The DRG and the spinal nerve sit within the IVF and are likely to be the source of pain and pathology when people suggest a 'radiculopathy' or 'nerve root compromise'. The dorsal spinal root comprises the trajectory of this axonal bundle between its entry into the cord and the intervertebral foramen (IVF). Shortly distal to the DRG, it fuses with the ventral spinal root to form the spinal nerve. Contrary to the DRG and the distal part of the dorsal root, both of which remain at the level of the IVF, the proximal part of the dorsal root lengthens considerably during development due to the ascensus of the cord. The more caudal the cord level, the longer the corresponding proximal dorsal root. The so-called root sheath covers this part of the dorsal root, which traverses the subarachnoid space to the cord. The latter is considered a continuation of both pia and arachnoid mater but possibly also of the deep perineurium (Feirabend HKP & Marani E 2003, in Encyclopedia of the Neurological Sciences)
Late in 2007, DeLeo, Sorkin & Watkins in their IASP publication Immune and glial regulation of pain devoted 5 chapters (of 23) to the DRG. Chapter 9 described DRG signaling and erythropoietin as a protective agent against neuropathic pain development (Campana, WM), chapter 10 cited the recognition that DRG satellite cells and trafficking leukocytes into the DRG may directly affect primary afferent signalling which enhances the complexity of glial - immune reactions within the CNS (McLachlan E). Chapter 21 described the ischaemic compromise due to the metabolic demands of immune - inflammatory processes in the DRG, as well as describing both pro-inflammatory (IL-1, IL-6, TNF-alpha) and anti-inflammatory (IL-10) cytokines found in the Nucleus Pulposus of the disk.
Sinuvertebral Nerve
Note that the sinuvertebral nerve (SNV) is a peripheral nerve that is 'recurrent'. It goes back into the IVF and presumably innervates those structures of the IVF as far centrally as the annulus fibrosis of the disc. The SNV, contains both somatosensory and sympathetic nerve fibres and therefore, has both somatic and visceral innervation functions. The innervation of the IVD is part of it's visceral function (Cavanaugh JM, et al 1997 Clin Orthop Relat Res. 335, 166-80). Although it passes through the intervertebral foramen, it is unlikely to be compressed during disc herniation because it is located alongside the pedicle, cranial to the corresponding disc. At the point of entrance, the composite nerve is about 0.5–1.0 mm in diameter. However, irritation of this nerve, presumably could be initiated by inflammation of the disc could initiate neurogenic inflammation, which in turn affects DRG function? Application of mechanical traction to this 'foramen' may aid in removing any irritation on the sinuvertebral nerve or the DRG, caused by inflammation and/or arterio-venous swelling.
The SNV also innervates a number of additional structures, one being the anterior portion of the dura mater within the spinal canal. Each sinuvertebral nerve sends a long descending meningeal branch that extends two segments caudally and a shorter ascending branch that traverses as far as one rostral segment. The plexus formed by the anastomoses of these branches covers the ventral surface of the dura mater and extends to the lateral aspects, but never reaches the dorsal surface, which remains devoid of nerve supply. The three most rostral sinuvertebral nerves ascend through the foramen magnum, at which point they innervate the dura mater covering the clivus within the posterior cranial fossa.
The sympathetic fibres carried in the SNV nerve are thought to innervate much of the surrounding vasculature, including the vessels that supply blood to the outer annulus, end plates, vertebral bodies, and marrow. It has been speculated that these fibres are primarily involved in vasomotor regulation, although some have been found to travel distal to the blood vessel, suggesting an additional undetermined function (Suseki K et al 1998 J Bone Joint Surg Br. 80, 4, 737-42)
Intervertebral Foramen

Note, the size of the IVF compared with it's contents (approx 30% is taken up by the contents). In the L5/S1 region some suggestions have been that 50% of the content is taken up. Additionally, there is a natural enlarging of the contents around the Dorsal Root Ganglion (DRG). Furthermore, the DRG is found in a transition zone, between the peripheral and central nervous systems. Presumably, this means that it receives it's nutrition, predominantly from the diffusion of nutrients in the cerebrospinal fluid (CSF) as well as potentially also from the peripheral vasculature of the IVF, controlled by the sinuvertebral nerve.
Peri-radicular injections
In the mid - late 1990's medical practitioners developed a methodology, for people with radicular pain, of injecting a cocktail of local anaesthetic and anti-inflammatory, around the nerve in the IVF. The results were quite amazing, whereby people who were previously destined for disc surgery, experienced considerable and long lasting relief of pain, as well as normalisation of neurological signs and symptoms. Initially, the mechanisms were unclear, however the clinical effects justified it's use.
The evidence for Transforaminal Epidural Steroid Injections (FESIs) reveals level III (moderate) evidence in support of these minimally invasive and safe procedures in treating painful lumbar radicular symptoms. Current studies support use of TFESIs as a safe and minimally invasive adjunct treatment for lumbar radicular symptoms (DePalma MJ et al 2005 Arch Phys Med Rehabil 86, 1477-1483). In another study, on spinal canal stenosis pain, of 68 patients with spinal stenosis, 22 (32%) had opted for surgery at two year follow-up. Thirty (44%) patients were satisfied with non-surgical management at 2 years, required no further treatment, and were discharged. Of the remaining 24%, nine patients were referred for further injection, four declined surgery but were referred to the Pain Relief Clinic, two still had a similar level of pain but declined surgery and one had died (Davis N et al 2017 Transforaminal epidural steroid injection in lumbar spinal stenosis: an observational study with two-year follow-up, British Journal of Neurosurgery, 31:2, 205-208, DOI: 10.1080/02688697.2016.1206188).
Similar to the need for 'specificity' in the application of Manual and Manipulative Physiotherapy, the judicious use of appropriately preformed injections can aid significantly in the ability to diagnose and treat patients with spine pathology. These are done with imaging guidance. To be appropriately therapeutic they must also be used in appropriately selected patients. When done appropriately these image-guided injections have a large body of literature demonstrating their efficacy for certain disease conditions (Schneider B.J., Varghis N., Kennedy D.J. (2016) Lumbar Spine Injections: An Evidence-Based Review. In: Pinheiro-Franco J., Vaccaro A., Benzel E., Mayer H. (eds) Advanced Concepts in Lumbar Degenerative Disk Disease. Springer, Berlin, Heidelberg. http://doi-org-443.webvpn.fjmu.edu.cn/10.1007/978-3-662-47756-4_33).
Theoretically, these effects are based on the removal of neurogenic inflammation and irritation in the IVF, as well as possible effects on the blood flow.
Contemporary Consideration of Dose of Lumbar Traction
As noted earlier, patients with acute lumbar sciatica secondary to disc herniation who received 2 weeks of lumbar traction, either at 10% BW or 50% BW, reported reduced radicular pain and functional impairment and improved well-being regardless of the traction force group to which they were assigned. The effects of the traction treatment were independent of the initial level of medication and appeared to be maintained at the 2-week follow-up. (Marie-Eve Isner-Horobeti et al 2016 J Manipulative Physiol Ther 39, 45-654)
Dosage of 30-50% body weight does not take into account the patients morphology (floppy vs stiffy), nor the state of their pathology. It has been hypothesised that, the high dose biomechanical construct (30-50% body weight), based on cadavers and anecdotal history (James Cyriax 1950's) of inter-vertebral separation, is much too high, if a neurophysiological approach is to be considered. By incrementally adding load, from 10->25kg, it can be noted, when a normalisation of signs and symptoms occurs. Moreover, at a certain point of loading, the signs and symptoms begin to deteriorate once again. It is considered, that this latter methodology, more appropriately takes into account, neurophysiological phenomenon such a neurogenic inflammation, deterministic chaos immunological responses, descending sympathetic as well as peripheral sympathetic nervous system responses as well as the need to clinically respect muscle spasm. Clinically, this has been a tried and tested method, where presumably a certain dose of traction takes pressure off the blood vessels and nerves inside the IVF and potentially stretches the capsule of the Z-joint, whereas a dose which is too large, stretches pain sensitive structures which re-invokes muscle spasms and re-introduces compression. Reflexogenic muscle spasms must be respected,

Force = the normalisation of S+S : Position = antalgic position, supine with legs in 90º flexion, supine with legs in slight flexion : Frequency = 1-2 times per week. Intermittent vs Constant = whatever feels best for the patient, however the clinician should be aware that I/T loading causes pre-conditioning and potentially greater creep and hysteresis.
Positioning
The position used, in mechanical traction, will reflect the stage, stability, severity and irritability of the condition, as well as investigating the position where normalisation of S+S occurs. Commonly, in the acute, severe stage of a condition, the position of comfort may be used. This may resemble the position in which the person sleeps. Frequently, positions such a lumbar spine rotation are used for the normalisation of S+S. Sometimes, combing positions, similar to those described clinically and biomechanically, by Brian Edwards and Freddy Kaltenborn, can be used with traction. Such clinical judgement calls, are frequently supported by the clinical reasoning process, rather than by clinical trials. Importantly, the application, of non-standard positions, can be used to 'load' or 'unload' spinal structure, thereby allowing the 'fine tuning' of dose.
Although the supine position is generally preferred, the client may also be positioned prone during traction treatment. However, few investigations, have compared the effects of lumbar traction in these two different positions for patients with chronic LBP. Investigators, divided participants.(n=125) randomly to receive 15 sessions of PT with additional mechanical lumbar traction either in the supine position (supine traction group), or in the prone position (prone traction group), or only PT without traction (PT only group). Subjects were assessed at baseline and at the end of the PT sessions in terms of disability, pain, and mobility. Disability was assessed using the modified Oswesty Disability Index (ODI); pain was assessed using a visual analogue scale (VAS); and lumbar mobility was assessed using the modified lumbar Schober test (mLST). These researchers found that the addition of traction in the prone position with other modalities resulted in larger immediate improvements in terms of pain and disability, and the results suggests that when using traction, prone traction might be first-choice. (Meral Bilgilisoy Filiz et al 2018 Ann Rheum Diseases 77 Suppl 2,:472.3-473 DOI: 10.1136/annrheumdis-2018-eular.1244 Conference: Annual European Congress of Rheumatology, EULAR 2018, Amsterdam, 13–16 June 2018)
On the other hand, other researchers compared static traction applied for 12 minutes at an intensity of 40% to 60% of the participant's body weight, with the McKenzie approach of treating people with LBP and leg pain. At the end of traction treatment, participants continued with the extension-oriented treatment approach (EOTA) component of treatment. They did not find superior results when adding traction to the EOTA (Thackeray, A et al (2016) JOSPT 46, 3, 144-154 https://www.jospt.org/doi/10.2519/jospt.2016.6238).
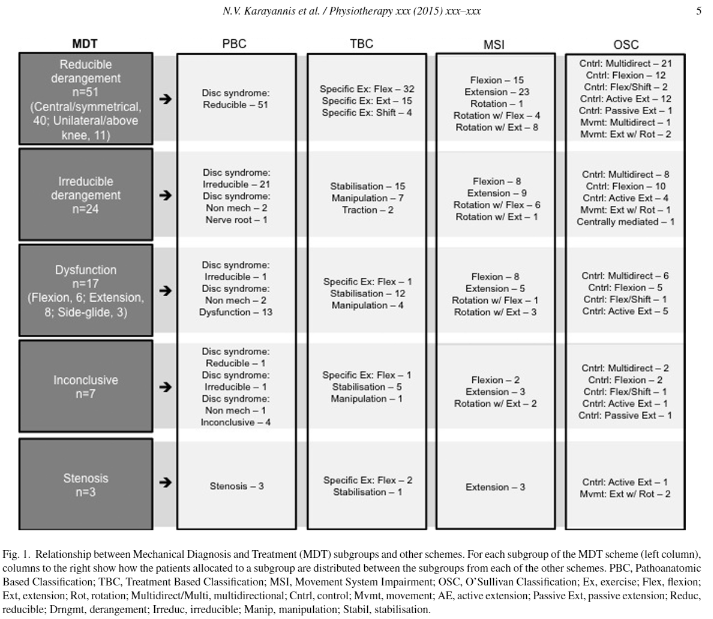
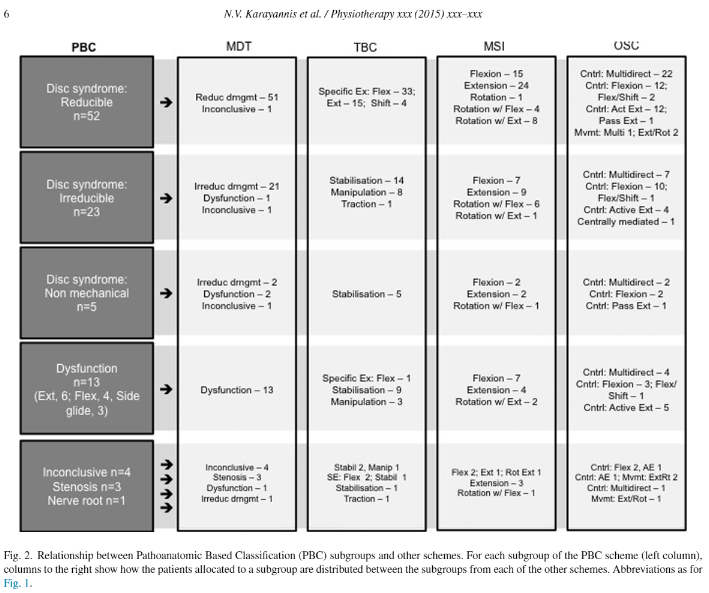
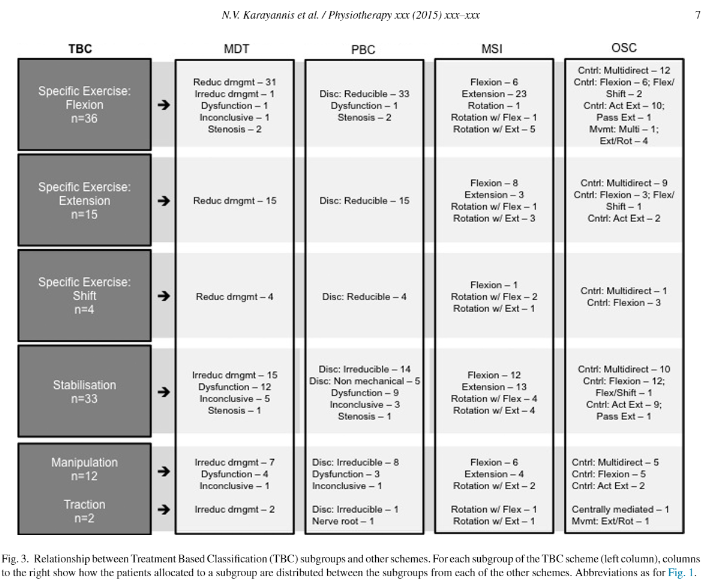
These dichotomous results may be due to high dosage used by Thackeray et al (2016). Interestingly, they did try to use clients use of movement into a pain relieving position, which would be a similar rationale for traction. Consensus amongst practitioners is to move into pain relieving positions when it's acute, severe and irritable. Later, in the sub-acute stages, non severe and non irritable it is desirable to move into pain provoking positions, if that results in normalisation of S+S. Direction of movement, is also a key aspect of Peter O'Sullivan's work and relates to several movement, treatment and mechanically based classification schemes (Karayannis NV, Jull G, Hodges PW (2015) Physiotherapy 102, 2, DOI: 10.1016/j.physio.2015.04.005)
Clinically, we generally consider whether a person stands in a posterior (decreased lordosis) or anterior (increased lordosis) pelvic position. Whether they have a passive extension pattern (sway back) or an active extension pattern ('tail in the air'). We also look at 'lists' generated by the lumbar spine and differentiate those from pelvic anomalies (inflare, outflare, upslip, downslip and counter-nutation).
Clinical Reasoning when Predicting Dose using Clinical Signs and Symptoms
Dosage needs to be predicted, clinically, through a thorough subjective examination, whereby the 'stage', 'stability', 'irritability' and 'severity' of the condition is determined prior to the physical examination. Early stage radiculopathy may only have low back pain, later stages may have no back pain and only leg pain, more severe conditions will have pins & needles or numbness, reduced muscle power, altered reflexes and altered neural tension signs such as limited straight leg raise (SLR). Resolving problems should be the reverse of this. However, some clients may feel they have improved or worsened relative to the irritability of their low back pain (LBP), completely disregarding numbness or other neurological signs. This is where the assessment and reassessment, provide the 'inflection point' (deterministic chaos) or the descending modulation needed, to create the 'fidelity', for determining what is and isn't normal and what does and doesn't improve the condition. In other words, the perception of the scope of the problem and the expectations of recovery need to be managed.
The 'stability' of the condition should be considered in terms of biomechanics, such as a spondylolisthesis, or in terms of the clinical condition, where a patients condition can easily swing back and forth between worsening and improving. I find in the latter, these people have either had some form of trauma, termed 'abuse' (in Geoff Maitland terminology) or in people who are generally hypermobile (Floppy) in conditions such as Ehlers Danlos Syndrome or Joint Hypermobility Syndrome (JHS). Other terminology used in the Geoff Maitland approach are 'misuse', 'overuse' and 'disuse' as causative factors. These causes should be entertained when establishing the appropriateness of mechanical traction as a treatment option, but also as a prognostic factor. Disuse, would suggest a person with little soft tissue resilience, overuse could suggest a fatigued and compromised immune system, whereas misuse could suggest serious cognitive descending motor control problems, including loss of cortical representation of muscles in the brain.
Inter - relationships between mobility and stability as they relate to clinical reasoning and function
Allostasis - the ability to switch on and switch off a neurophysiological - immune response to a given 'stressor'
The physical examination can be used for immediate feedback to determine dose
The presence of Clonus or Babinski reflex is an absolute contra-indication to traction, as it is highly indicative of cord or cauda equina compression, which generally requires an immediate surgical consult. In some very few cases the presence of these signs are, instead, due to higher neurological compromise such as stroke, head trauma and drug abuse.
Mechanisms of Action
It has been demonstrated, using CT scans, that during traction ( distraction force of 45 kg, for twenty minutes), the area of the spinal canal, and the width of the neural foramen increased 21.6%, and 26.7% respectively. Furthermore, an average of 3:3 +/- 1:9 mm (1.9%) expansion of the lumbar column length was measured (Sari H et al, 2005 Physiotherapy Theory and Practice, 21, 1, 311). They also noted that the predominant effect of disc resorption occurred more in central protrusions and to a much lesser extent in posterolateral herniations. Presumably, the posterior longitudinal ligament is involved here. Furthermore, they described greater distraction in the posterior elements of the spine. These results used high dose traction. Unfortunately, these researchers didn't compare the results of incremental loading. However, as previously described low dose traction demonstrate similar clinical results, compared with higher doses.
Through the normalisation of muscle spasm, the amount of 'force closure' around the spine should reduce. Consequently, such a reduction in muscle tension should reduce compressive forces on the intervertebral discs (IVD) and blood vessels of the intervertebral foramen (IVF) as well as the spinal canal (Batson's venous plexus).
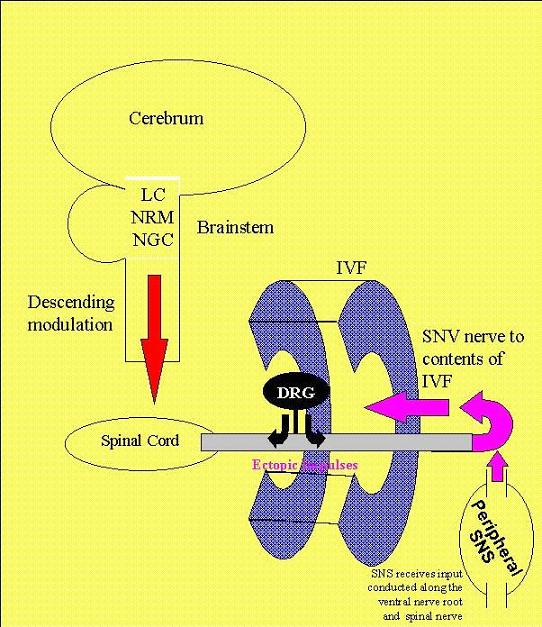
Normalisation of pressure around the dorsal root ganglion (DRG) should reduce the propagation of ectopic impulses to the spinal cord and moreover improve the afferent-efferent interaction in the periphery. It is hypothesised that the latter would improve the modulation of blood flow as well as the modulation of neurogenic inflammation. It should be remembered that the sinuvertebral nerve (SNV) is a peripheral nerve responsible for these effects within the intervertebral foramen and spinal canal.

Even momentary normalisation of 'ectopic inputs', from pain and inflammation, as well as improved vascularisation and/or reduced oedema, may have a lasting effect on neuroplasticity, similar to when local anaesthetic, applied peri-radicularly, can have a long lasting effect, beyond the pharmacological washout period. Additionally, the post-traction procedure of re-establishing normal muscle synergy, around the pelvis, thorax and the spine, during a pain free period, may also be just enough stability needed to support, and thereby 'unload' injured structures.
Neurophysiology of Pain and Inflammation
Sympathetic-sensory coupling after L5 spinal nerve lesion in the rat and its relation to changes in dorsal root ganglion blood flow
H. -J. Haebler, S. Eschenfelder, X. -G. Liu and W. Jaenig (October 2000).
Abstract
Transection of the L5 spinal nerve in rats results in allodynia- and hyperalgesia-like behaviour to mechanical stimulation which are thought to be mediated by ectopic activity arising in lesioned afferent neurons mainly in the dorsal root ganglion (DRG). It has been suggested that the neuropathic pain behaviour is dependent on the sympathetic nervous system. In rats 3–56 days after L5 spinal nerve lesion, we tested responses of axotomized afferent fibres recorded in the dorsal root of the lesioned segment to norepinephrine (NE, 0.5 g/kg) injected intravenously and to selective electrical stimulation of the lumbar sympathetic trunk (LST). In some experiments we measured blood flow in the DRG by laser Doppler flowmetry. The majority of lesioned afferent fibres with spontaneous activity responded to neither LST stimulation (82.4%) nor NE (71.4%). In those which did react to LST stimulation, responses occurred only at high stimulation frequencies (likely to be above the physiological range), and they could be mimicked by non-adrenergic vasoconstrictor drugs (angiotensin II, vasopressin). Excitatory responses to LST stimulation were closely correlated with the stimulation-induced phasic vasoconstrictions in the DRG. We therefore hypothesized that the activation of lesioned afferents might be brought about indirectly by an impaired blood supply to the DRG. To test this hypothesis we induced a strong and sustained baseline vasoconstriction in the DRG by blocking endothelial nitric oxide synthesis with N G -nitro- -arginine methyl ester ( -NAME) applied systemically. -NAME enhanced baseline vascular resistance in the DRG about threefold and also increased stimulation-induced vasoconstrictions. After -NAME, the majority of axotomized neurons with spontaneous activity were activated by LST stimulation (76%) or NE (75%). Again, activations closely followed stimulation-induced phasic vasoconstrictions in the DRG provided that a critical level of vasoconstriction was exceeded. In the present study, inhibitory responses to LST stimulation were generally rare and could be reversed to activation by prolonged stimulation or after -NAME. These results show that sympathetic-sensory coupling occurs only in a minority of axotomized afferents after L5 spinal nerve injury. Like previous studies, they cast doubt on the notion that the L5 spinal nerve lesion is a good model for sympathetically maintained pain. Since responses of lesioned afferent neurons to LST stimulation and NE could be provoked with high reliability after inducing vasoconstriction in the DRG, and since they mirrored stimulation-induced vasoconstrictions in the DRG, it appears that in this model the association of sympathetic activity with afferent discharge occurs mainly when perfusion of the DRG is impaired.
If one considers the sinuvertebral nerve to be a peripheral nerve then induction of inflammation around the DRG can in turn create changes within the DRG which leads to hyperalgesia. Clearly a vicious cycle may ensue.
Induction of high mobility group box-1 in dorsal root ganglion contributes to pain hypersensitivity after peripheral nerve injury
Pain, 149, 3, 514-521
Masayuki Shibasaki1, Mika Sasaki1, Mayumi Miura1, Keiko Mizukoshi1, Hiroshi Ueno, Satoru Hashimoto, Yoshifumi Tanaka, Fumimasa Amaya
Abstract
Pro-inflammatory cytokine high mobility group box-1 (HMGB-1) is involved in inflammation in the central nervous system, but less is known about its biological effects in the peripheral nervous system. In the present study, the role of HMGB-1 in the primary afferent nerve was investigated in the context of the pathophysiology of peripheral nerve injury-induced pain hypersensitivity. Real-time PCR confirmed an increase in HMGB-1 mRNA expression in the dorsal root ganglion (DRG) and spinal nerve at 1day after spinal nerve ligation (SNL). Induction of HMGB-1 mRNA was observed in both injured L5 and uninjured L4. Immunohistochemistry for HMGB-1 revealed that SNL-induced HMGB-1 expression in the primary afferent neurons and satellite glial cells (SGCs) in the DRG, and in Schwann cells in the spinal nerve. Up-regulation of HMGB-1 was associated with translocation of its signal from the nucleus to the cytoplasm. Injection of HMGB-1 into the sciatic nerve produces transient behavioural hyperalgesia. Neutralizing antibody against HMGB-1 successfully alleviated the mechanical allodynia observed after SNL treatment. Receptor for advanced glycation end products (RAGE), one of the major receptors for HMGB-1, was expressed in the primary afferent neurons and SGCs in the DRG, as well as in Schwann cells in the spinal nerve. These results indicate that HMGB-1 is synthesized and secreted into the DRG and spinal nerve, and contributes to the development of neuropathic pain after nerve injury. Blocking HMGB-1/RAGE signalling might thus be a promising therapeutic strategy for the management of neuropathic pain.

Paradigm shift
A lot has been learnt since first writing on the mechanisms of mechanical traction. In 1994, the treatment was considered almost entirely from biomechanical point of view. A passive modality applied to an inert structure. I argued, that the descending modulation of what I then termed 'neurogenic inflammation' was critical to outcome and that the 'window of dosage', like the Goldilocks story, 'of getting it just right' meant that neither the application nor the objective of that application were 'passive'. Unfortunately, the semantics of the time were a considerable impediment to progress. They directed treatment at the 'nerve root', even though anatomically it resides in the spinal canal rather than the IVF. Physiotherapists applied 'passive joint mobilisations', they did 'manual therapy', to 'collagen'. Although, this was the case, the collagen turned out to possess remarkable neurophysiological properties, as they were innervated, the other soft tissue, such as myofascia turned out to have fibroblasts which could move around the body, as well as being endowed with a very rich immune ecology. Furthermore, muscle was considered merely as a thing which could contract and be stretched. More enlightened manual therapists (Jenny McConnell) considered their neurological training and incorporated theories of motor control (Janet Carr and Roberta Shepard). In 1986, I wrote of muscle synergies, (around the knee and shoulder) using a perspective of nett motor control around an inflection point and that any disruption, either through weakness and/or muscle spasm would disrupt the controlling mechanism at the inflection point. By 2002 I was writing about muscle as an endocrine organ. In 2020, I am writing about the muscle-gut-brain axis as an immune organ whose complexity is regulated by deterministic chaos around similar inflection points. Interested readers on pain and motor control should look elsewhere on this site : https://www.back-in-business-physiotherapy.com/physiotherapy-teaching/motor-control-of-the-cervical-and-lumbar-spine.html
Those interested in muscle synergies across the pelvis should look at : https://www.back-in-business-physiotherapy.com/we-do/muscle-energy-techniques.html
Chaos, Exercise and the Immune Systems : https://www.back-in-business-physiotherapy.com/health-advocacy/exercise-and-the-immune-system-during-covid-19.html
Myofascial substance release with dry needling : https://www.back-in-business-physiotherapy.com/we-do/dry-needling.html
Target organ of traction - IVF or the IVD?
Essentially, there is nothing 'passive' about manual therapy and it is one of the reasons, why 'double blind' 'controlled' designed investigations, failed so spectacularly, to establish efficacy, back in the 1990's. It's impossible to include a 'placebo' group when active engagement, with the patient, is crucial to outcome. Additionally, if the 'outlier' determines the effect (see deterministic chaos link above), by defining what it is not, then patient specific treatment tailored not to their pathology, but to the stage, stability, irritability and severity of the disorder is mandatory. As such, identification of patient specific sub-groups has to be determined, if scientific investigations into efficacy, are to be undertaken. I argue that, the appreciation of the possible localised mechanism of action, can be used, as a 'bottom - up approach', to the establishment of construct and face validity, for the justification of using mechanical traction in the treatment of certain LBP.
The obsession with the Intervertebral Disc (IVD), as the target organ of traction, is disingenuous, to all of the structures which compromise the IVF. In fact, what if traction fails when it's targeted at the IVD? Peri-radicular injections are often effective at normalisation of S+S, where, it is plausible that, the target of such injections, is not just the IVD, but all the richly innervated contents and structures of the IVF. Importantly, the poorly innervated and non-innervated IVD is highly unlikely to have an immune-neurophysiological mechanism of recovery. Where these injections and traction may fail, could be where, rather than the consequences of the IVD pathology being the target organ, it's the IVD itself, which is really the over-riding pathology, where surgical intervention may be required. Hence, these are different clinical pictures, derided from the clinical reasoning approach, to LBP management. Hence, sub-groups need to be identified, both clinically and during research, when efficacy is being established.
The model depicted above is a summarised version of the original treatise written in 1995. Just as relevant today as it predicted what scientific endeavours would find. Luckily, the understanding and semantics have changed, however, it still hasn't resulted in robust trials, using lower doses, to demonstrate favourable outcomes. Please see below for a more detailed theoretical explanation.
Altered proprioception and perception - dura mater and adverse neural tension
It is plausible that traction provides a unique stimulus to the spinal canals dura mater. Normally, when we bend forward, the posterior aspect of the dura mater 'unfolds', similarly when we bend back, it's the anterior aspect and sideways the contralateral side. However, mechanical traction may give the brain, the perception of simultaneous movement in all directions, thereby relaxing muscles to allow movement to occur. Additionally, this longitudinal stimulus may stimulate the peripheral sympathetic ganglia, producing an autonomic response. Regardless, clinically, the range of movement in side bending and rotation of the thorax frequently improve. Additionally, side bending of the cervical spine also frequently occurs. So much so, that I am frequently using lumbar spine mechanical traction whilst simultaneously mobilising the cervical spine and upper thoracic rings.
In the past neural tension tests were considered to be a stretch on the sciatic or femoral nerve adjacent to the contents of the IVF. However, we know that, the irritation of inflamed tissues, causes reflexogenic muscle spasms which, for Straight Leg Raise (SLR), results in reduced movement, in the spine (Erector Spinae and Multifidus) but also at the the hip (Piriformis), Knee (Hamstring) and ankle (Calf). This scenario has to be differentiated from the more 'severe' form where serious nerve compression results in extreme weakness in those muscles.
Soft Tissue Biomechanical Considerations of Lumbar Traction
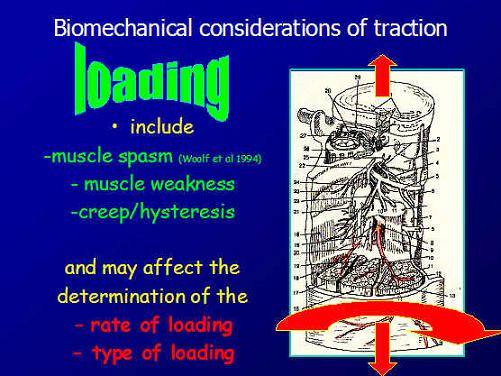
In terms of soft tissue biomechanics, it can easily be imagined, that a 'floppy' person will react differently than a 'stiffy', with greater 'creep' and 'hysteresis' in the former. Additionally, the age of the tissue may also need consideration, as the nucleus pulposus of the disc becomes more fibrous in the fourth decade of life. Also, a person with some excessive 'joint play' (functional instability), increased neutral zone, will also have different biomechanical considerations. Structural instability is an absolute contra-indication to this form of traction.
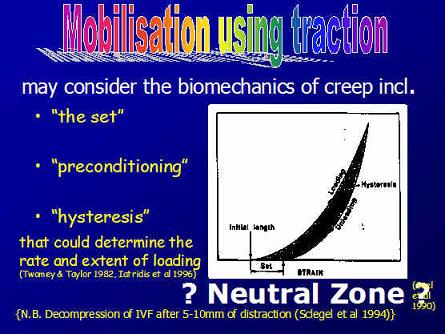
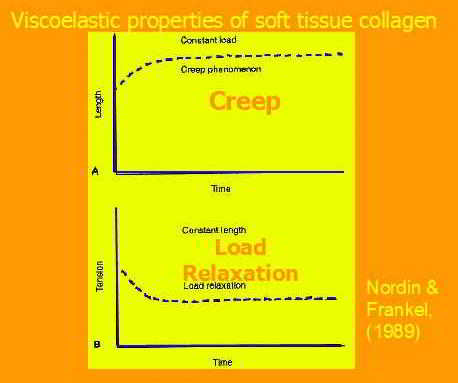
A frequent consideration when dosing traction is whether an intermittent or constant load should be used. Generally, in the acute phase a constant force is used, whereas at later stages intermittent loading may be more desirable. In a stiff person, the I/T load may result in greater displacement, thanks to a phenomenon called 'pre-conditioning'. Other reasons for using I/T loading is because the person states that they don't like to be still or where the therapist thinks that movement will encourage blood flow.
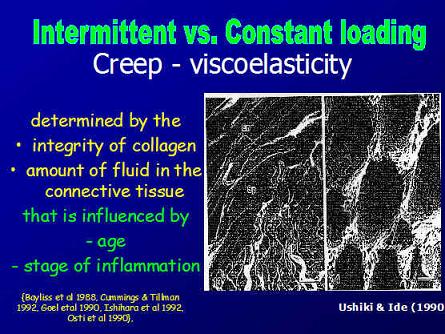
Additional, important considerations are a persons collagen type, where some people and races (e.g. Asian and African) are predisposed to hypermobility, whereas others have stronger and stiffer collagenous integrity (floppy vs stiffy).
Placebo versus Nocebo effect
As alluded to previously, the nervous system must become engaged in the treatment process. This can go in either two ways, one which has a positive therapeutic outcome, based on interactions in the brain resulting in amelioration of signs and symptoms, or a negative effect which some people have referred to as a 'nocebo'. By writing this, it might imply that all musculoskeletal physiotherapeutic interactions are either a placebo or nocebo. This is not what I wish to say. However, I would like to suggest that semantics can be highly deleterious to our thinking as applied scientists and clinicians. There is a plethora of evidence which demonstrates that higher cognitive engagement needs to exist for a successful outcome. See the previous link, given above, for further information.

Nocebo could be termed the neurophysiological and behavioural effect which occurs, when there is no discernible improvement in the patients condition, from the intervention performed. Conditioned and unconditioned stimulus inputs converge on individual cells in the lateral amygdala, which is the principal output nucleus, of the fear system, which projects to areas of the hypothalamus and brainstem, that control behavioural, endocrine, and autonomic conditional responses, associated with fear learning (Goldstein JA 2004). In neurosomatic disorders, an accentuation of the attentional weighting is given to elements of a stimulus that, in actuality, have a very tenuous relationship to the state of activation of the long-term memory store. Unlike the individual with a normally functioning neural network for associated learning, the activated memory store to which the stimulus is associated does not rapidly decay but continues to be highly weighted, even if this weighting is outside the individual's attention (Newport DJ, Nemeroff CV 2000; in Goldstein JA 2004).
Fear and Learning
Attentional resources are allocated in favour of unexpected salient events. The term 'switching' is used to denote reallocation processes, and 'salient' is used to refer to stimuli with special biological significance. Dopaminergic output is involved in 'behavioural orienting', the allocation of attention to a particular stimulus. This response normally extinguishes rapidly. Unexpected rewards or punishments lead to the acquisition of new conditioned responses. Dopaminergic activity is suppressed when expected rewards fail to materialize. Basal ganglia have evolved to resolve conflicts of multiple subsystems competing for access to limited motor or cognitive resources ( see orienteering section of website for more details ). The frontal eye fields brings visual stimuli into the most active perceptual area of the retina, so it's potential reward significance can be determined. The computations of the possible reward occur before the behavioural switch occurs, and a signal is often lost before the identity of the stimulus is fully known (Goldstein JA 2004).
The prefrontal cortex (PFC) and noradrenergic systems are both important for attentional regulation. Lesions of the PFC impair the ability to sustain attention to relevant information and to inhibit processing of irrelevant stimuli. Neurones in the locus coereleus (LC) fire in relation to the attentional state, and the PFC is one of the few high-order inputs to the LC and is an important regulator of it's activity. Noradrenaline is known to enhance signal-to-noise ratio in sensory cortices. With insufficient noradrenergic stimulation, small signals may be obscured (targets) while potent stimuli may be processed (distractors). If noradrenaline is hypersecreted, it would take the PFC 'off line'. The PFC may be responsible for exploratory responses in a fear-inducing environment (Goldstein JA 2004). Therefore, higher centres are most probably involved in assessing the visual input during the assessment of signs and symptoms. Immediate demonstration of clinical improvement, or otherwise, has salient implication on the higher centre processing of pain and inflammation.
Mechanisms of placebo analgesia: rACC recruitment of a subcortical antinociceptive network
U. Bingel et al (2006) Pain, 120, 1-2, 8-15
Abstract
Placebo analgesia is one of the most striking examples of the cognitive modulation of pain perception and the underlying mechanisms are finally beginning to be understood. According to pharmacological studies, the endogenous opioid system is essential for placebo analgesia. Recent functional imaging data provides evidence that the rostral anterior cingulate cortex (rACC) represents a crucial cortical area for this type of endogenous pain control. We therefore hypothesized that placebo analgesia recruits other brain areas outside the rACC and that interactions of the rACC with these brain areas mediate opioid-dependent endogenous anti-nociception as part of a top–down mechanism. Nineteen healthy subjects received and rated painful laser stimuli to the dorsum of both hands, one of them treated with a fake analgesic cream (placebo). Painful stimulation was preceded by an auditory cue, indicating the side of the next laser stimulation. BOLD-responses to the painful laser-stimulation during the placebo and no-placebo condition were assessed using event-related fMRI. After having confirmed placebo related activity in the rACC, a connectivity analysis identified placebo dependent contributions of rACC activity with bilateral amygdalae and the periaqueductal gray (PAG). This finding supports the view that placebo analgesia depends on the enhanced functional connectivity of the rACC with subcortical brain structures that are crucial for conditioned learning and descending inhibition of nociception.
Dissection of perceptual, motor and autonomic components of brain activity evoked by noxious stimulation
Pichéacef M et al (2010) Pain, 149, 3, 453-462
Abstract
In the past two decades, functional brain imaging has considerably advanced our knowledge of cerebral pain processing. However, many important links are still missing in our understanding of brain activity in relation to the regulation of pain-related physiological responses. This fMRI study investigates the cerebral correlates of pain (rating), motor responses (RIII-reflex) and autonomic activity (skin conductance response; SCR) evoked by noxious electrical stimulation. Stimulus intensity was adjusted individually based on the RIII threshold to control for differences in peripheral processes and baseline spinal activation. Covariance analyses were used to reveal individual differences in brain activity uniquely associated with individual differences in pain, RIII and SCR. Shock-evoked activity in cingulate, medial orbitofrontal and para-hippocampal regions predicted pain sensitivity. Moreover, lateral orbitofrontal and cingulate areas showed strong positive associations with individual differences in motor reactivity but negative associations with autonomic reactivity. Notably, individual differences in OFC activation was almost fully accounted by the combination of individual measures of autonomic and motor reactivity (R2=0.93). Additionally, trial-to-trial fluctuations of RIII-reflex and SCR (within-subjects) were proportional to shock-evoked responses in sub-genual cingulate cortex (RIII), anterior insula (SCR) and midcingulate cortex (SCR and RIII). Together, these results confirm that individual differences in perceptual, motor, and autonomic components of pain reflect robust individual differences in brain activity. Furthermore, the brain correlates of trial-to-trial fluctuations in pain responses provide additional evidence for a partial segregation of sub-systems involved more specifically in the ongoing monitoring, and possibly the regulation, of pain-related motor and autonomic responses.
The Neuromatrix
According to Melzack (1999) the sensory-discriminative, affective-motivational and evaluative-cognitive dimensions of pain experience are determined by the multiple inputs that act on the neuromatrix programmes. These include sensory inputs, visual inputs which influence the cognitive interpretation of the situation, phasic and tonic cognitive inputs from other areas of the brain, intrinsic neural inhibitory modulation, activity of the body's stress-regulation systems including cytokines, as well as endocrine, autonomic, immune and opioid systems. Therefore, the role of mechanical traction within a multi-modal approach would be a useful clinical research paradigm.
Clinical Reasoning Approach
An Integrated Approach
One of the biggest impediments to the use of mechanical traction, using the two threshold hypothesis, is having the client understand the meaning of improved reflexes and power or range of movement of neural tension signs. Geoff Maitland used to hypothesis that the appropriate dose was when the persons pain level was 50% of what they originally felt. Pain is just one variable in the clinical presentation. Only useful when considered in the total clinical picture. Unfortunately, clients often have an expectation, that traction will have a similar sensation to when they are stretching muscles. As we all know, back muscles are very difficult to stretch. They lie very close to their axis of rotation and generally aren't stretched in activities of daily living. Furthermore, mechanical traction is a novel stimulus. We don't normally experience an anti-gravity pull in the longitudinal axis of the spine. Hence, I frequently apply traction to howls of protest that they "cannot feel anything". Through the normalisation of signs and symptoms, this sentiment needs to be adjusted.
Perception is everything. Both for the therapist and client, perceptive awareness is a pathway for learning and discovery. An integrated multi-modal treatment model was developed for the multi-dimensional pain management problem. Again, this flies in the face or reductionist principles. However, it does highlight the use of the integrated and most effective use of various manual therapy and clinical reasoning techniques to deride an optimal outcome.
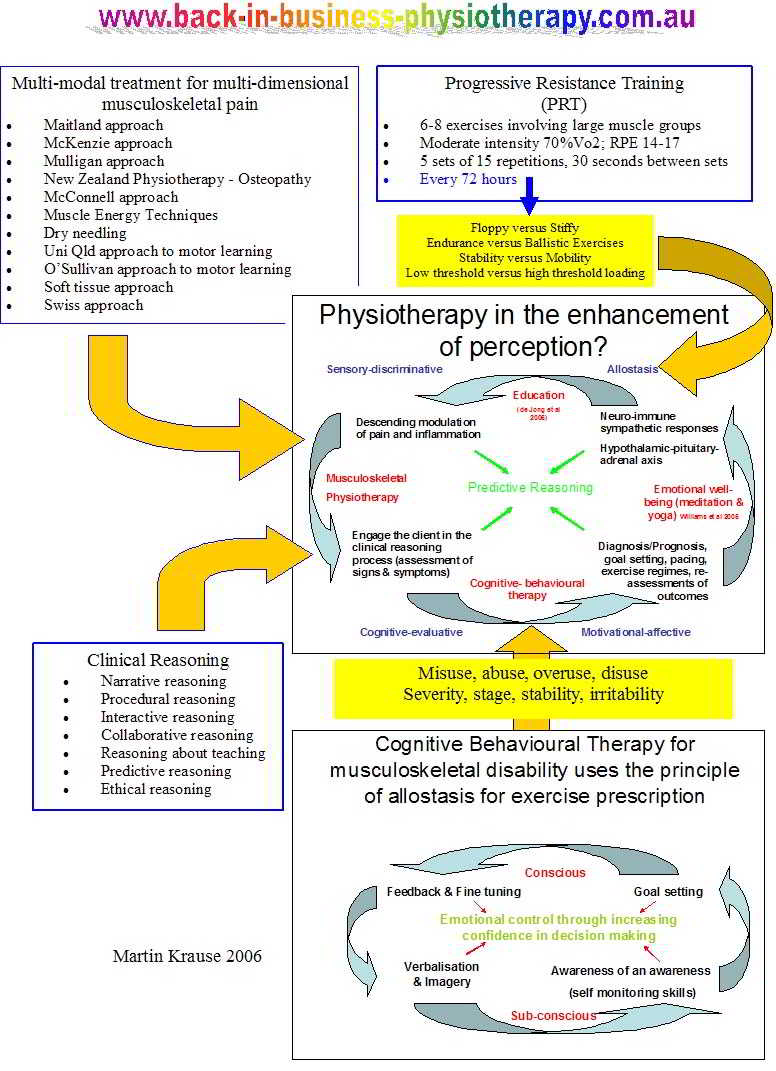
Multi-modal approach to treatment of multi-dimensional musculoskeletal conditions.
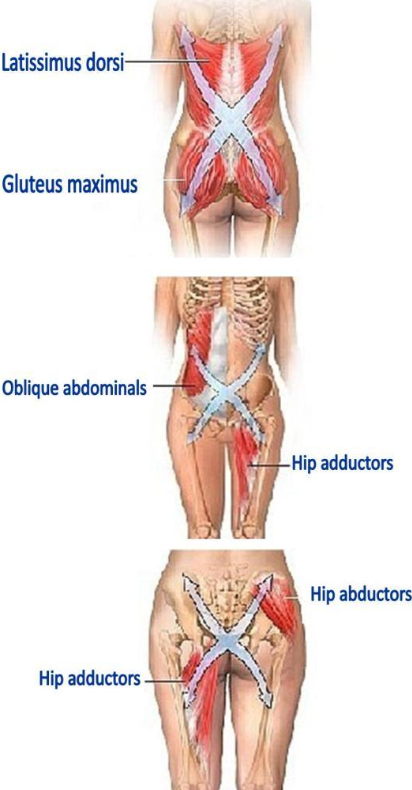
Generally, my treatment approach may use a number of techniques, prior to the administration of traction. These can include manual therapy and muscle energy techniques around the hip and pelvis, thoracic ring relocation techniques, dry needling and myofascial release of the mid to low thoracic regions as well as Psoas Major releases. Mechanical traction can be used as a uni-modal self standing technique. However, acting as a sling and creating a scenario of improved muscle strength and/or reduced muscle spams, means that reduced splinting or stability, needs a methodology, whereby the muscle sling synergy is re-established immediately, after the application of traction. Hence, a series of exercises are given as the person lies on the traction table (abdominal exercises, bridges, spinal rolling), as they sit up (buttock clenches, abdominal exercises) and after they stand up ('wall plank', ROM, 'queen mum' and 'hammer head'). This may be even more important for the 'floppy' (hyper-mobile) person or in any scenario where an increased 'neutral zone' exists?
Muscle Slings and the 're-setting' of muscle synergies.
Once mechanical traction force has finished, the normal protocol involves allowing the client to rest for 5 minutes with traction bed closed. Then a gradual and progressive re-establishment of muscle synergies is commenced in s systematic way, progressing from the treatment position, to different positions on the bed, then sitting and eventually standing. Hereby, allowing the client to engage a natural corset of muscle synergies before they even get dressed.
Andre Vleeming came up with a concept that the bones of the body sit in a sling of muscles, meaning that these structures are loaded and unloaded by synergistic muscle actions. This includes the active muscle contractile components as well as the myofascia. Tensegrity has also been used to describe this biomechanical phenomenon at a macro and micro-structural level. A big argument against the effectiveness of mechanical traction is the one that the disc is unloaded and once treatment is finished and the person stands up, the disc is re-loaded. It is argued that, rather than the disc, it's the contents of the IVF (and Z-joint swelling) which is 'unloaded' and that it's the re-establishment of muscle synergies which maintains this unloaded state.
Various muscle exercises can be seen in the rock climbing section of this website
Chronic Stress
Chronic stress may have a direct influence on pain.
Increased basal mechanical pain sensitivity but decreased perceptual wind-up in a human model of relative hypocortisolism
Linn K. et al (2010) Pain, 149, 3, 539-546Abstract
Clinical data have accumulated showing that relative hypocortisolism, which may be regarded as a neuroendocrinological correlate of chronic stress, may be a characteristic of some functional pain syndromes. However, it has not been clarified yet whether deregulations of the hypothalamus–pituitary–adrenal (HPA) axis may directly alter pain perception and thus be causally involved in the pathophysiology of these disorders. To test this hypothesis, we performed a randomized placebo-controlled crossover trial in N=20 healthy drug-free volunteers (median age 24yrs) and analysed the effects of metyrapone-induced hypocortisolism on quantitatively assessed basal mechanical pain sensitivity (1.5–13m/s impact stimuli), perceptual wind-up (9m/s impact stimuli at 1Hz) and temporal summation of pain elicited by inter-digital web pinching (IWP; 10N pressure stimuli for 2min). Experimentally induced hypocortisolism significantly decreased pain detection thresholds and augmented temporal summation of IWP-induced pain (p<.05). The latter effect was dependent on the relative reduction in cortisol levels, and seemed to rely on a potentiated sensitization and not merely on the observed changes in basal pain sensitivity. Perceptual wind-up by contrast was reduced when cortisol synthesis was blocked (p<.05). This result is reminiscent of findings from animal studies showing a reversal of NMDA receptor activation by glucocorticoid receptor antagonists in neuropathic pain models. Our results speak in favour of a potential causal role of HPA axis alterations in pain chronicity.
Descending Modulation of Pain

Context and Meaning
WDR = Wide Dynamic Range , NS + Nociceptive Specific, PAG = Peri Aqueductal Grey matter in the brainstem
Further information on Pain in the Brain can be found elsewhere on this website
Patient Feedback
Examination Process
The examination process is designed to "make the features fit" into a meaningful clinical picture whereby a diagnosis and prognosis can be made. If the therapist cannot explain to the client what the problem is, then we have a problem. Most (99%) of our daily cognitive processing occurs at a subconscious level. By activating the auditory process of inductive and deductive reasoning, the therapist can avoid the trap, of missing vital information, which differentiates this persons unique problem from another person. It also, encourages and engages the client in the reasoning process.
The therapist should be 'reductionist', commencing with a multitude of 'filtering' questions, which guides the physical examination and in turn creates a basis on which to not only formulate an intervention strategy, but also results in a mechanism, whereby the results of treatment can be determined. This structured process is clinical, as well as scientific, in that it sets a 'null hypothesis' (diagnosis) and predicts an outcome. When the expected outcome isn't forthcoming, then a re-evaluation and re-questioning and re-examination of the condition is required, a new intervention strategy created and potential referral to another professional considered. All along, carefully monitoring and potential deterioration of the condition, and in particular, re-evaluation of the neurological signs and symptoms is required.
Possible Effects of Traction
The Two Threshold Hypothesis
The 2 threshold hypothesis of dose suggests that a therapeutic dose (normalisation of signs and symptoms) for lumbar spine traction occurs at a very low threshold of around 12-14kg and another threshold occurs with a deterioration of signs and symptoms at around 20-25kg. These values vary to some extent depending on the stage, stability, irritability and stability of the disorder, as well as the persons soft tissue morphology (floppy vs stiffy)..
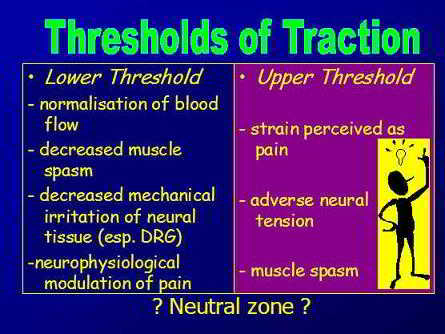
The lower threshold relieves pressure on the contents (nerve and blood vessels) of the IVF, whereas the upper threshold places tension on structures which comprise the surroundings of the IVF. These surroundings include the annulus fibrosis of the disc, the z-joint capsule and various ligaments and potentially even some adverse tension on the peripheral sympathetic ganglion chain.
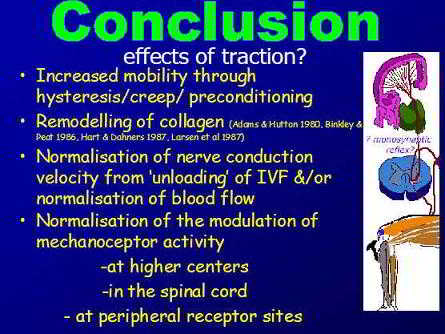
Conclusion
Therefore, it appears to be important to engage the client in the clinical reasoning process. In so doing, they are not passive recipients of treatment. Rather, their cognitive processes are involved with the aims and objectives of treatment as well as expected outcome. Additionally, their motor systems are involved not only in the re-evaluation of signs, but also in the re-establish of correct muscle co-ordination and stability post traction. Importantly, general consensus suggests that multi-modal treatment approaches within the clinical reasoning frame of reference is more efficacious than using one modality alone. Hence, treatment with mechanical traction should be integrated with other techniques such as joint mobilisations of the hip & thoracic spine, muscle energy techniques, soft tissue massage, trigger point massage, fascial release, dry needling, taping, and exercise regimes appropriate for the stage, stability, severity, & irritability of the disorder, whilst respecting biomechanical principles of inverse dynamics.
For more information on Musculoskeletal Low Back Pain and treatments LBP Treatment Progress.
It should be noted however, that patients who have high scores on the Catastrophizing Scale of the CSQ (Coping Strategies Questionnaire : Rosentiel & Keefe 1983), who endorse passive coping strategies on the PMI (Pain Management Inventory : Brown et al 1989), who demonstrate low self efficacy regarding their ability to manage their pain on the PSEQ (Pain self efficacy questionnaire : Lorig et al 1989), who describe themselves as disabled by their pain on the SOPA (Survey of pain attitudes : Jensen et al 1987), and who report negative thoughts about their pain on the INTRP (Inventory of negative thoughts in response to pain : Gil et al 1990) are at greatest risk for poor treatment outcome (Jamison 2004).
Overall, it can be concluded that a 'two threshold mechanism' exists for a sub-group of patients. The immune-neurophysiological consequences of the IVD hernia, on the structures of the IVF and it's contents, are indeed an important target of treatment, using mechanical traction. Loading greater than a 'tolerable threshold' probably affects the IVD and the PLL and it's Batsons Venous Complex, where neurological S+S deteriorate. It's the historic bias towards the IVD model, as an inert poorly innervated structure, requiring some arbitrary, clinically unproven, high loading (30-50% BW), that is potentially dangerous, and hence should not be used clinically, which has stifled many clinical trials and research. Further research, needs to identify and monitor the normalisation of neurological S+S, as the 'null hypothesis', rather than using an unproven biomechanical bias.
Further evidence regarding psychological aspects of pain and impaired brain processing come from the following recent investigations :
Chronic pain patients are impaired on an emotional decision-making task
Vania Apkarian et al (2004) Pain, 108, 129-136
Abstract
Chronic pain can result in anxiety, depression and reduced quality of life. However, its effects on cognitive abilities have remained unclear although many studies attempted to psychologically profile chronic pain. We hypothesized that performance on an emotional decision-making task may be impaired in chronic pain since human brain imaging studies show that brain regions critical for this ability are also involved in chronic pain. Chronic back pain (CBP) patients, chronic complex regional pain syndrome (CRPS) patients, and normal volunteers (matched for age, sex, and education) were studied on the Iowa Gambling Task, a card game developed to study emotional decision-making. Outcomes on the gambling task were contrasted to performance on other cognitive tasks. The net number of choices made from advantageous decks after subtracting choices made from disadvantageous decks on average was 22.6 in normal subjects ( n =26), 13.4 in CBP patients ( n =26), and -9.5 in CRPS patients ( n =12), indicating poor performance in the patient groups as compared to the normal controls ( P <0.004). Only pain intensity assessed during the gambling task was correlated with task outcome and only in CBP patients ( r =-0.75, P <0.003). Other cognitive abilities, such as attention, short-term memory, and general intelligence tested normal in the chronic pain patients. Our evidence indicates that chronic pain is associated with a specific cognitive deficit, which may impact everyday behaviour especially in risky, emotionally laden, situations.
Dimensions of catastrophic thinking associated with pain experience and disability in patients with neuropathic pain conditions.
Michael J.L. et al (2005) Pain, 113, 310-315
Abstract
The objective of the present study was to examine the relative contributions of different dimensions of catastrophic thinking (i.e. rumination, magnification, helplessness) to the pain experience and disability associated with neuropathic pain. Eighty patients with diabetic neuropathy, post-herpetic neuralgia, post-surgical or post-traumatic neuropathic pain who had volunteered for participation in a clinical trial formed the basis of the present analyses. Spontaneous pain was assessed with the sensory and affective subscales of the McGill Pain Questionnaire. Pinprick hyperalgesia and dynamic tactile allodynia were used as measures of evoked pain. Consistent with previous research, individuals who scored higher on a measure of catastrophic thinking (Pain Catastrophizing Scale; PCS) also rated their pain as more intense, and rated themselves to be more disabled due to their pain. Follow up analyses revealed that the PCS was significantly correlated with the affective subscale of the MPQ but not with the sensory subscale. The helplessness subscale of the PCS was the only dimension of catastrophizing to contribute significant unique variance to the prediction of pain. The PCS was not significantly correlated with measures of evoked pain. Catastrophizing predicted pain-related disability over and above the variance accounted for by pain severity. The findings are discussed in terms of mechanisms linking catastrophic thinking to pain experience. Treatment implications are addressed.
Self-management of chronic pain: a population-based study
Fiona M. et al (2005), Pain, 113, 285-292
Abstract
While effective self-management of chronic pain is important, clinic-based studies exclude the more typical pattern of self-management that occurs in the community, often without reference to health professionals. We examined specific hypotheses about the use of self-management strategies in a population-based study of chronic pain subjects. Data came from an Australian population-based random digit dialling computer-assisted telephone survey and included 474 adults aged 18 or over with chronic pain (response rate 73.4%). Passive strategies were more often reported than active ones: passive strategies such as taking medication (47%), resting (31.5%), and using hot/cold packs (23.4%) were most commonly reported, while the most commonly reported active strategy was exercising (25.8%). Only 33.5% of those who used active behavioural and/or cognitive strategies used them exclusively, while 67.7% of those who used passive behavioural and/or conventional medical strategies did so exclusively. Self-management strategies were associated with both pain-related disability and use of health services in multiple logistic regression models. Using passive strategies increased the likelihood of having high levels of pain-related disability (adjusted OR 2.59) and more pain-related health care visits (adjusted OR 2.9); using active strategies substantially reduced the likelihood of having high levels of pain-related disability (adjusted OR 0.2). In conclusion, we have shown in a population-based study that clinical findings regarding self-management strategies apply to the broader population and advocate that more attention be given to community-based strategies for improving awareness and uptake of active self-management strategies for chronic pain.
Also see the following investigations into the role of neuro-immune substances in pain modulation
Tumour necrosis factor alpha and interleukin-1ß stimulate the expression of cyclooxygenase II but do not alter prostaglandin E 2 receptor mRNA levels in cultured dorsal root ganglia cells
Jill C. et alAbstract
Tumour necrosis factor alpha (TNF-alpha) and interleukin 1ß (IL-1ß) are pro-inflammatory cytokines capable of altering the sensitivity of sensory neurons. Because sensitization elicited by IL-1ß and TNF-alpha is blocked by inhibition of the inducible enzyme, cyclooxygenase-II (COX-2), we examined whether these cytokines could increase COX-2 expression in dorsal root ganglion (DRG) cultures. Treatment of cell cultures with either IL-1ß or TNF-alpha increases immuno-reactive COX-2, as measured by immunoblotting, in a time- and concentration-dependent manner. A 24-h pre-treatment with 10 ng/ml IL-1ß or 50 ng/ml TNF-alpha augmented COX-2 expression 50- and 8-fold over basal levels, respectively. Immunohistochemistry established the presence of COX-2-like immunoreactivity in both neuronal and non-neuronal cells in culture. The addition of IL-1 receptor antagonist blocked the induction of COX-2 expression by IL-1ß, but did not alter TNF-alpha-stimulated increases in COX-2, indicating that the mechanism of TNF-alpha is not limited to increasing the expression of IL-1ß. The basal and TNF-alpha-induced expression of COX-2 was not dependent on the presence of NGF in the growth media. IL-1ß and TNFalpha treatment for 24 h enhanced prostaglandin E 2 (PGE 2 ) production 2–4-fold, which was blocked by pre-treatment with the COX-2 inhibitor, NS-398. Exposing cultures to PGE 2 , IL-1ß, or TNF-alpha for 24 h did not alter PGE 2 receptor (EP) mRNA levels. These results indicate that TNF-alpha and IL-1ß induce the functional expression of COX-2 but not EP receptors in DRG cells in culture and suggest that cytokine-induced sensitization of sensory neurons is secondary to prostaglandin production and not alterations in EP receptors.
Excitatory and modulatory effects of inflammatory cytokines and neurotrophins on mechanosensitive group IV muscle afferents in the rat
Hoheisel U et al Link to Pain Journal
Abstract
In inflamed tissue – including skeletal muscle – the concentrations of cytokines and neurotrophins are known to increase. However, nothing is known about a possible contribution of these agents to muscle pain and hyperalgesia. The present study investigated acute effects of cytokines and neurotrophins on response properties of slowly conducting muscle afferents. In anaesthetised rats, the impulse activity of single mechanosensitive group IV fibres innervating the gastrocnemius–soleus muscle was recorded and tumour necrosis factor-alpha (TNF-alpha), interleukin-6 (IL-6), nerve growth factor (NGF), or brain-derived neurotrophic factor (BDNF) were injected into the muscle. Changes in the mechanosensibility of the endings following administration of the agents were tested with repeated pressure stimuli of defined forces. A low mechanical threshold in the innocuous range was found in 44.4% of the units tested, 55.6% required strong, potentially tissue-damaging pressure stimuli for activation. NGF excited only units that had a high mechanical threshold, while IL-6 was a stimulant for low-threshold mechanosensitive units only. TNF-alpha and BDNF did not excite group IV units but had a desensitising action: after TNF-alpha or BDNF, the response magnitudes to pressure stimuli decreased significantly. The data indicate that cytokines and neurotrophins influence the impulse activity and mechanosensitivity of group IV muscle afferent units. These effects could be of functional significance when the agents are released from muscle cells under pathophysiological circumstances.
Spinal nerve lesion-induced mechanoallodynia and adrenergic sprouting in sensory ganglia are attenuated in interleukin-6 knockout mice
Matt S. et al. link to Pain Journal
Abstract
Tight ligation and transection of the L5 spinal nerve (SNL) gives rise to pain which is dependent upon activity in the sympathetic nervous system. It also results in novel adrenergic sympathetic innervation of the dorsal root ganglion (DRG) with the formation of pericellular axonal basket structures around some DRG neurons. Since the sympathetic sprouting and basket formation may represent an anatomical basis for pain-generating interactions between the sympathetic efferent neurons and sensory afferent neurons, it is of great interest to determine possible chemical mediators of this phenomenon. Previous findings have shown that IL-6 can contribute to sympathetically-independent pain, and can give rise to thermal hyperalgesia when injected intrathecally. We have now investigated a possible contributory role of the pleiotropic cytokine interleukin-6 (IL-6) in sympathetically-mediated pain: we gave IL-6 knockout mice and mice of the parent strain c57B6/129 a SNL, assessed their resulting pain behaviour for 10 days post-surgery, and used tyrosine-hydroxylase immunohistochemistry to compare sympathetic sprouting in the DRG at the end of the testing period. We found that thermal allodynia (as assessed by measuring the latency to withdrawal from radiant heat) did not differ significantly between strains. On the other hand, in the IL-6 mice, mechanoallodynia (as assessed with von Frey filaments) was markedly delayed. Sympathetic invasion of the fibre tract and cell layer of the DRG, and the formation of pericellular axonal baskets were all significantly reduced in the IL-6 knockout mice compared to the control strain. These results imply a facilitory role for IL-6 in pain and sympathetic sprouting induced by nerve injury, and add to the growing list of roles for IL-6 in neuropathological events.
Clinical example using mechanical traction
Presentation on Stress, Exercise and the Immune System
Mechanical traction - a neurophysiology explanation was conceptualised and conceived predominantly during early 1995 as part of my Masters treatise at Sydney University - for references see below as well as the paper on pain and inflammation elsewhere on this site.
Additional References
Melzack R (1999) From the gate to the neuromatrix. Pain Supplementation 6; S121-S126
Newport DJ, Nemeroff CB (2000) Neurobiology of post traumatic stress disorder. Current Opinion in Neurobiology 10; 211-218
Goldstein JA (2004) Tuning the Brain. Principles and practice of neurosomatic medicine. The Hawthorn Press New York
Grossberg S (2000). The complimentary brain: unifying brain dynamics and modularity. Trends in Cognitive Sciences 4, 233-246
The Construct Validity for Considering the Dorsal Root Ganglion (DRG), the Intervertebral Foramen (IVF) in Musculoskeletal Physiotherapy Reasoning
by Martin Krause, 1995 & 2000.
SUMMARY
The efficacy of manual therapy interventions has been extensively criticised in recent years. Serious charges of physiotherapy induced conviction of disease (nocebo) leading to chronicity have been raised. Paradoxically, the omission of higher centre processing in the design of double blind investigations, results in a dichotomy of interpretation which, either justifies the determination of inefficacy or alternatively, predicts an important role for higher centre involvement during the selection and application of manual therapy techniques. Specifically, the sensory-discriminative and motivational-affective responses require dissemination if hypotheses regarding the efficacy of manual therapy treatment, for acute radicular pain, are to be made. Currently, the majority of pain research has established immune-nervous system responses associated with post-traumatic inflammation rather than repair. Recently, dysfunction of the dorsal root ganglion (DRG), which lies in the intervertebral foramen (IVF), has been implicated in both the genesis and chronicity of radicular pain. Previously, manual therapy techniques to the IVF, such as traction, have been anecdotally advocated to normalise signs and symptoms in acute radicular pain. Clinicians use the presenting signs and symptoms, to guide their clinical reasoning processes. Additionally, the normalisation of signs and symptoms is used to demonstrate the usefulness of a treatment technique to their clients. Investigations demonstrate higher centre involvement in the reduction of pain and inflammation. Clearly, if the efficacy of manual therapy is to be determined, then the differentiation between a treatment dependent descending inhibition of pain and inflammation, with that of a placebo or nocebo, is required.
INTRODUCTION: HIGHER CENTRE SENSORY-DISCRIMINATIVE AND MOTIVATIONAL-AFFECTIVE SENSORY PROCESSING BY THE NERVOUS SYSTEM
Recently, sensory-discriminative (Ploner et al. 1999) and motivational-affective (Vogt et al 1993) pathways for pain have been demonstrated in humans. The main constituents of the sensory-discriminative aspects of pain (Aδ fibre activity) include the lateral thalamic, primary (I) and secondary (II) somatosensory cortices. Conversely, the motivational affective aspects of pain consists predominantly of the medial thalamic nuclei and the anterior cingulate cortex. Importantly, this structural differentiation suggests that the specificity of treatment and the demonstration of efficacy are important aspects in the nervous systems responses to treatment. Frequently, the practitioner uses the normalisation of signs and symptoms to demonstrate efficacy, in addition to guiding their clinical reasoning processes (Higgs & Jones 1995). However, such an approach could be dangerous as it reinforces the conviction of disease and could result in a nocebo effect (Bogduk 1997; Cohen 1995). Hence, what role does the sensory-discriminative aspect of pain have on the motivational-affective response to manual therapy techniques?
Positron Emission Tomography (PET) has demonstrated that higher centres of the nervous system may be actively involved in, the descending inhibition of acute pain and inflammation in humans (Hsieh et al. 1995; Petrovic et al. 1999). Animal investigations of supraspinal opioids found a block in the perception of pain, through a 64% reduction in superficial laminae dorsal horn activity (Gogas et al. (1991) (usually associated with a predominance of nociceptive specific neurones {Lima et al. 1994}), and a 85% reduction in ventral horn activity (usually associated with motor neurones) in animals (Schomburg & Steffens 1991). One source of descending inhibition involves pontine noradrenergic projections, in animals (Janig 1985; Martin et al. 1999; Post et al. 1986; Morgan et al. 1989; Nakagawa et al. 1990; Ren et al. 1990; Proudfit 1992). Although descending noradrenergic inhibition is considered to be an opioid-independent form of analgesia (Proudfit 1992), evidence supports the view that m-opioid and a-2 noradrenergic receptors are functionally linked to pain modulation (Gebhart et al 1994). Higher centres have been implicated in sympathetic responses, to spinal manual therapy techniques, in humans (Petersen et al. 1993; Vicenzino et al. 1998). Plausibly, the sensory-discriminative pathway was involved in the reduction of secondary hyperalgesia, as these techniques were applied to the neck for lateral elbow pain.
Evidence for important motivational-affective responses are from animal investigations which, substantiate the finding that higher centres can act in an antinociceptive manner (Sandkuehler et al. 1995). Importantly, a "behavioural set" has been defined as 'a state of readiness or preparation to receive a stimulus that has not yet arrived, or a state of readiness or preparation to make a movement' (Woodworth 1958 c.f. Dubner & Ken 1999). Therefore, the net effect of descending inhibition in animals from the Locus Coeruleus/Subcoeruleus, Nucleus Raphe Magnus, and Nucleus Gigantocellularis is to "dampen or counteract the cascade of events that ultimately lead to the development of inflammatory hyperalgesia" (Dubner and Ken 1999) (see figure 1). Attention and cognitive factors such as previous experience of manual therapy or possibly even the apparent normalisation of signs and symptoms could modulate noxious stimuli in the primary somatosensory cortex (Bushnell et al. 1999; Dubner & Ken 1999). These motivational-affective responses presumably occur with the interaction of the client and the therapist during the clinical reasoning process.
Together, these investigations represent very powerful arguments for assessment of the signs and symptoms during the clinical reasoning process, thereby involving higher centres in the neuromodulation of pain and inflammation. Additionally, the activation of higher centres through the re-setting of stabilising muscles, after the person receives passive joint mobilisation treatment, may be necessary for even greater involvement of higher centres. Confirmation of motivational-affective responses to treatment would require the use of psychometric pain questionnaires, positron emission tomography (PET) and functional MRI to demonstrate the temporal changes in cerebral activity (Casey & Minoshima 1997; Svensson et al. 1997) before, during and after treatment
ECTOPIC IMPULSE GENERATION IN THE DORSAL ROOT GANGLION (DRG) AND NEUROGENIC INFLAMMATION IN THE SENSORY NERVE ENDINGS OF THE SINUVERTEBRAL (SNV) NERVE – A ROLE FOR LOCALISATION OF TREATMENT?
To justify an important localised sensory-discriminative response to injury and hence treatment requires an appreciation of dorsal root ganglion (DRG) dysfunction. Inflamed structures demonstrate increased excitability of sensory nerve endings (Raja et al. 1988; Schmidt et al. 1994). A cause of acute radicular spinal pain may be the generation of excessive electrical activity (ectopic impulses) from inflamed structures. Passive joint mobilisations may be useful in the treatment of radicular spinal pain by 'unloading' those structures (e.g. DRG) whose functions include the modulation of ectopic impulse generation. Ectopic discharge can occur in the DRG following damage that occurs distally in the neural pathway and in the presence of endoneural oedema in animals (Howe et al. 1977), and humans (Nordin et al. 1984). Essentially, endoneural oedema of the DRG resulting from compression by extraneural inflammatory exudate (Chatani et al. 1995) in the intervertebral foramen (IVF) generates ectopic electrical impulses (Bandalamente et al. 1987). These ectopic impulses originating in the DRG are thought to propagate into the spinal cord and into peripheral receptor sites (Wall & Devor 1983; Bandalamente et al. 1987). Consequently, the extent of spinal cord sensitisation, oedema and neurogenic inflammation may in some cases be more significant than the physical size of an intervertebral disc (IVD) protrusion (Garfin et al. 1991; Thelander et al. 1992). Interestingly, Bogduk (1997) advocates radiofrequency neurotomy in the treatment of chronic spinal pain. However, in acute radicular pain it becomes apparent that the DRG is likely to regulate the excitability of the sensory nerve endings (Devor 1999). Therefore, 'unloading' of mechanical compromise (extraneural inflammation) around the DRG in the IVF, by for example traction, could plausibly reduce ectopic impulse generation (see figure 2).
Ectopic impulse generation from the DRG may propagate throughout the innervation of the sinuvertebral (SNV) nerve. The SNV nerve is a peripheral nerve formed by the recurrent branch of the ventral ramus and a branch of the grey ramus communicantes of the somatic and peripheral sympathetic nervous systems respectively (Bogduk & Twomey 1997). Since the SNV nerve does not innervate superficial structures of the body, it may play a sensory-discriminative role such as mechanoception and nociception (Ahmed et al. 1993). Certainly, the types of receptors innervating the ligamentous structures, suggests such roles (Korkula et al. 1985; Weinstein et al. 1988a). Similar to other peripheral nerves, a vasoactive role on blood vessels may be a function of the sympathetic component of the SNV nerve (Appenzeller et al. 1984; Selander et al. 1985; Weinstein et al. 1988b; Zochodne et al. 1990). Importantly, the terminals of the SNV nerve appear anatomically well placed to transmit ectopic impulses to the IVD, posterior longitudinal ligament, Hoffman ligaments, and the dura mater (Weinstein et al. 1988a, Bogduk & Twomey 1997). This increased ectopic impulse propagation increases neurogenic inflammation, possibly at the SNV nerve receptor sites (Markowitz et al. 1989; Xavier et al. 1990; Chatani et al. 1995). Arborization of the SNV nerve terminals can cause neurogenic inflammation in an expanded receptive field (LaMotte et al. 1991). Furthermore, expansion of spinal cord neuronal hypersensitivity may arise from the propagation of ectopic impulses into the spinal cord from the periphery (Wall & Devor 1983). This expansion is called secondary hyperalgesia and possibly explains the severity of referred limb pain, which is a frequent manifestation of radicular pain. Therefore, a dual role of the SNV nerve in the detection of nociception, in addition to the propagation of ectopic impulses to structures of the IVF and spinal canal is plausible. Presumably, specific manual therapy techniques will induce a sensory-discriminative response, which is likely to activate a motivational-affective response that either increases or decreases secondary hyperalgesia depending upon the perceived appropriateness of the treatment.
THE HYPOTHESIS: SPINAL TECHNIQUES AFFECT THE DORSAL ROOT GANGLION (DRG) IN THE INTERVERTEBRAL FORAMEN (IVF)
Clearly the expansion of the hypersensitive receptive field, underlie the importance of investigating the sensory-discriminative aspects of treatment techniques. Variation of techniques to the IVF, such as the type of load (stretch vs. compression, active vs. passive), the position, and the duration are probably detected by SNV nerve terminals, innervating inflamed structures. Since the SNV nerve appears to innervate the DRG itself (Cuartico et al. 1988; Groen et al. 1988), the ramifications of extraneural inflammation in the IVF are vascular compromise inducing intraneural oedema in the DRG. Consequently, intraneural oedema causes ectopic impulse generation, which increases the intensity of the existing extraneural neurogenic inflammation. Hence, an ongoing self-perpetuating cycle of neurogenic inflammation ensues, which potentially impoverishes any regulation in excitability of sensory nerve endings by the DRG. Thus, if a treatment technique affects the vascular compromise (and extraneural inflammation) surrounding the DRG, in the IVF, then a resultant reduction in endoneural oedema in the DRG would interrupt this self-perpetuating cycle of neurogenic inflammation. Significantly, reduced ectopic impulse generation and enhanced modulation of excitability of sensory nerve endings, by the DRG, may substantiate the validity of using the immediate normalisation of signs and symptoms for the determination of the appropriate technique (Larsson et al. 1980; Maitland 1986; Eggertz 1986; Pal et al. 1986; Knutsson et al. 1988) (see figure 3). Thus, any measured changes in sensory-discriminative function may imply an activation of higher centre responses. In turn, the subsequent motivational-affective response may be indirectly determined through autonomic testing of that innervation field (Sandroni 1998).
A MODEL: MECHANICAL TRACTION FOR THE NORMALISATION OF SIGNS AND SYMPTOMS IN ACUTE RADICULAR SPINAL PAIN
A recent review suggested some people with acute radicular spinal pain responded well to traction with the normalisation of signs and symptoms (Krause et al. 2000). Specifically, to determine an important sensory-discriminative response then the predictive validity of the current model is the normalisation of signs and symptoms within a narrow band of loading tolerance. Since the valid dose of traction would be the normalisation of signs and symptoms, then the inappropriate dose will be the deterioration of signs and symptoms. In considering ectopic impulse generation, 'unloading' of the contents of the IVF (i.e. Nerve Root/Dorsal Root Ganglion/Spinal Nerve, intra-foraminal blood vessels, sinuvertebral nerve) may be a logical explanation for the first observation of the normalisation of signs and symptoms. Reduction in ectopic impulse generation and simultaneously enhanced modulation of inflammation could be expected from the mechanical 'unloading' of the DRG in particular. Similarly, if the inflamed structures comprising the IVF (i.e. IVD, Zygapophyseal joint, Hoffman ligaments, etc) (Groen et al. 1988; Park & Watanabe 1990; Wiltse et al. 1993; Bogduk & Twomey 1997) are 'overloaded', then ectopic impulse generation (Raja et al. 1988; Schmidt et al. 1994) with the deterioration of signs and symptoms can be expected during excessive traction. The normalisation-deterioration of signs and symptoms can be referred to as a two-threshold hypothesis.
The clinical implications of the sensory-discriminative and motivational-affective aspects of pain highlight the importance of differentiating a specific neurophysiological effect from the placebo and nocebo. Clearly the demonstration of efficacy and expectations of outcome are an essential aspect of any treatment protocol. Presumably, some people will deteriorate or not respond to traction at all. In these people, the loading threshold has not been reached or another form of treatment is more appropriate. Importantly, lack of improvement or deterioration may induce a nocebo response. Therefore, the clinical reasoning process needs to identify the responders from the non-responders in a manner, which expedites appropriate treatment. Hence, a correlation with psychometric questionnaires and the temporal aspects of functional MRI and PET diagnostic imaging would be required before conclusions of efficacy are drawn. Since it is unlikely that a person could guess their threshold for their normalisation of signs and symptoms, then a method of investigation for a differentiation of the neurophysiological, placebo and nocebo effect may include the use of the two-threshold hypothesis.
THE VALIDITY OF USING THE NORMALISATION OF SIGNS AND SYMPTOMS
The validity of testing procedures underlie the ability of the examiner to make a clinical prediction (Payton 1988). Clinical reasoning uses signs and symptoms to determine the appropriateness of a treatment strategy (Higgs & Jones 1995). However, is the reduction in ectopic impulse generation and the modulation of excitability in sensory nerve endings correlated with the observable normalisation of signs and symptoms? Significantly, the incidence of the normalisation of signs and symptoms is not clear. Therefore, is the normalisation of signs and symptoms useful for making consistent decisions on the appropriateness of treatment technique for acute radicular pain? Finally, does the use of this methodology impart conviction of disease?
The pain response and range of motion (ROM) of straight leg raise (SLR) is a variable used to assess the effects of treatment using traction (Larsson et al. 1980; Eggertz 1986; Mathews et al. 1987; Pal et al. 1986; Tesio et al. 1989). The load and position of the patient have been defined by the improvement in the pain free ROM of SLR (Larsson et al. 1980). During SLR, the direct contact pressure of the DRG against the structures of the IVF (Smith et al. 1993) and tension generated in inflamed nerve roots are thought to cause sufficient ectopic impulse generation to stimulate the reflexogenic drive to the alpha-motor neurones, as demonstrated in animals (Woolf et al. 1994). Clinically, this reflexogenic drive may represent increased muscle activity that reduces ROM. Since ectopic impulse generation from the DRG also propagates into the spinal cord, then neuronal hypersensitivity could explain alterations in signs and symptoms on the contralateral side seen in humans and animals (Larsson et al. 1980; Woolf 1984; Woolf & Swett 1984; Woolf & MacMahon 1985; Woolf & Wall 1986b; Schmidt 1990; Eckert et al. 1999). Confirmation of such findings require, fine needle electromyography (EMG). Obviously, solely comparing ROM of SLR to the opposite side without due consideration of other variables may lead to errors in the clinical reasoning process.
Other variables inferring some validity when correlated with the normalisation of SLR, during treatment, include reduction in pain intensity, normalisation of muscle strength, and restoration of somatosensory evoked potentials (Knutsson et al. 1988). Additionally, improved asymmetric skin temperatures and sensation testing has been demonstrated (Knutsson et al. 1988; Onel et al. 1989). Although, the incidence of the normalisation of signs and symptoms was high, methodological problems exist which suggest caution in the interpretation of these results. Never the less, normalisation of muscle power, skin sensation, skin temperature, and pain intensity may be correlated with ROM of SLR to predict appropriate technique during the clinical reasoning process.
Normalisation of tendon reflexes has been used to assess patients, during auto-traction, and is thought to correlate with the normalisation of conduction along nerve fibres (Larsson et al. 1980; Pal et al. 1986; Knutsson et al. 1988; Onel et al. 1989; Sabbahi & Khalil 1990b). However, hypersensitivity in spinal cord reflexes can cause tendon reflexes to increase or decrease during neurogenic inflammation and ectopic impulse generation (Ferrell et al. 1988; Rees et al. 1994). Evidence for variable hyper- and hyporeflexia during inflammation comes from Hoffman-reflex investigations where increasing stimulus intensity increases the reflex until a given stimulus threshold is reached where a decrease or complete block in the Hoffman-reflex amplitude occurs (Sabbahi & Khalil 1990a). Since inflamed tissues have reduced receptor threshold, then excessive electrical activity during loading may alter reflex activity (Raja et al. 1988). Whether the hypersensitivity of spinal cord reflexes from neurogenic inflammation and ectopic impulse generation represent a decrease rather than an increase in tendon reflex awaits confirmation in the clinical situation. Importantly, this stimulus-dependent phenomenon may explain the deterioration of signs and symptoms when a technique is applied indiscriminately. Paradoxically, rather than demonstrating efficacy, such sensory-discriminative methodology has been seen to impart conviction of disease, which negatively influences the motivational-affective aspects of the pain (Bogduk 1997: Cohen 1995, Zusman 1998). Therefore, clinical reasoning based upon the normalisation of signs and symptoms would only be justified if a reduction in chronicity could be demonstrated. Epidemiology, using large numbers of subjects, would be required to validate these opinions.
RESTORATION OF NERVE CONDUCTION THROUGH THE MODULATION OF NEUROGENIC INFLAMMATION AND CYTOKINE-IMMUNE RESPONSES BY THE DRG AND PERIPHERAL SYMPATHETIC NERVOUS SYSTEM (SNS)
Peripheral nerve injury results in morphological changes in the DRG (Dib-Hajj et al. 1999; Eckert et al. 1999; Ramer et al. 1999). Although these morphological changes relate to chronic constriction, the onset and perpetuation of neurogenic inflammatory responses appear to begin within hours of the acute phase of injury (Schmidt et al. 1994). Notably, the SNV nerve and spinal nerve may represent the peripheral nerves susceptible to constriction irritation. The proposed genesis of these morphological changes are Wallerian degeneration in the periphery releasing nerve growth factor, leukaemia inhibitory factor and Interleukin (IL) - 6 (Ramer et al. 1999). The activation of similar cytokines is also associated with immune responses during exercise induced musculoskeletal damage (Pedersen et al. 1999) (SEE : Immune function and muscle mass or slide presentation for more detail). The disruption of the fibroblast endothelium is considered the 'trigger' for the release of tumour necrosis factor, IL-1, IL-6, IL-8. Subsequently, there is an activation of prostaglandin driven release of Substance P, with its consequential further release of cytokines from macrophages and mast cells, which completes a self-perpetuating cycle of inflammation (Groenblad et al. 1991; Rothwell & Hopkins 1995). Generally, inflammation and mast cell degranulation affects blood-nerve permeability and nerve conduction (Harvey et al. 1994). If, the interaction between the DRG and peripheral SNS is responsible for these immune responses during inflammation, then a treatment technique like traction may aid in reducing constriction of the affected peripheral nerves. In turn, the re-establishment of DRG function will enhance the modulation of cytokine activity. It is difficult to conceive any methodology, which may directly image these morphological changes in humans. Interestingly, some of the resultant restitution of nerve conduction is predicted to occur beyond the immediate application of the treatment technique. Therefore, the extent by which manual therapy techniques can prevent such morphological changes from occurring could justify early and appropriate treatment interventions. Certainly, pharmacological investigations have demonstrated greater treatment efficacy when early intervention was instigated (Bhala et al. 1988).
REDUCTION OF VENOUS CONGESTION AND THE MODULATION OF HOMEOSTASIS BY THE DRG IN THE INTERVERTEBRAL FORAMEN (IVF).
Reduction in mechanical irritation from venous congestion around the DRG may be an explanation for the efficacy of a treatment technique such as traction. Cadaveric studies demonstrate that mechanical abnormalities within the spine, such as IVD extrusion, result in dilatation, congestion, and thrombosus of veins contributing to disruption of the vascular endothelium and consequent fibrin deposition (Hoyland et al. 1989). Importantly, intraforaminal blood flow may represent part of the sensory-discriminative function of the DRG. The unusual location of the DRG between the peripheral and central nervous systems has been related to its hypothesised function as a sensor of background information such as homeostasis of the IVF milieu (Devor 1999). Besides location, evidence supporting a homeostatic function of the DRG is the lack of blood-nerve barrier around the cells of the DRG and the highly convoluted nature of its vasculature (Devor 1999). Obviously, sufficient blood flow would be required to detect homeostasis. Arguably, techniques such as traction achieve reduction in mechanical irritation by increasing the space for the intra-foraminal blood vessels of the IVF. Apparently, improved IVF space has been demonstrated by merely positioning a person to reduce their lumbar lordosis (Panjabi et al. 1983). The implications are that the function of the DRG may be susceptible to vascular and mechanical compromise in the IVF. Since venous pressure is quite low, the advocacy of using positions of comfort in acute radicular pain may be justified (Maitland 1986), as the required restitution of homeostasis in the IVF may occur.
Additional explanations for the effectiveness of using the 'positions of comfort' or low dose traction reside in the effect of neural irritation from compression at two locations. Besides swelling in the IVF from inflammatory exudate, the zygapophyseal (Z) joint may be swollen and inflamed. Histological changes suggestive of inflammation have been demonstrated in the Z-joint (Cooper et al. 1995). Since the Z-joint represents the posterior aspect of the IVF then presumably some decompression of the IVF may result from stretching of the Z-joint capsule during traction (Krause et al. 2000). Interestingly, nutrient transport to the nerve roots from both the intraneural blood vessels and from diffusion from the cerebrospinal fluid is affected in the intermediate zone between the two sites of compression almost as much as at the compression sites themselves, in rats. Even low pressure (10mmHg) is sufficient to induce a significant reduction in total blood flow possibly from retrograde capillary stasis due to venous occlusion (Rydevik et al. 1984a,b; Olmarker et al. 1989a,b; Cornefjord et al. 1992; Matsui et al. 1992; Takahashi et al. 1993). Clinically, pressure from extruded IVD material, in the IVF, and swelling of the Z-joint may represent a similar situation to the animal model. Importantly, relatively small traction loads or 'positions of comfort' may be required to reduce compromise at one site, thus resulting in the restoration of venous flow necessary for any homeostatic function of the DRG in the IVF. Perhaps, ultrasound imaging may be useful for demonstrating alterations in the dimensions of the Z-joint capsule. Certainly, ultrasound has been effective in demonstrating changes to the size or shape of the multifidus muscle which inserts into the Z-joint capsule (Hides et al. 1994). MRI of the IVF, doppler ultrasound of intraforaminal flow and computer modelling may be investigative procedures, of the future, for determining the biomechanical response to the treatment technique.
HEALING: THE ROLE OF THE VASCULATURE AND PERIPHERAL SYMPATHETIC NERVOUS SYSTEM IN THE MODULATION OF NEUROGENIC INFLAMMATION AT THE SINUVERTEBRAL (SNV) NERVE TERMINALS: A MOTIVATIONAL – AFFECTIVE RESPONSE TO SOMATOSENSORY STIMULI?
The sympathetic efferents are postulated to be important to the healing process since the activation of peripheral terminals of sympathetic postganglionic neurones contributes to neurogenic inflammation (Levine et al. 1986). Since emotions and somatosensory inputs profoundly influence the autonomic nervous system, non-invasive autonomic testing has been advocated in people with pain (Sandroni 1998). Sympathetic postganglionic neurones release inflammatory mediators that increase plasma extravasation, including prostaglandins (Coderre et al. 1989; Gonzales et al. 1989; Gonzales et al. 1991; Green et al. 1991a,b). Additionally, under conditions of sympathetic postganglionic neuronal modulation, bradykinin has been found to increase plasma extravasation (Green et al. 1992). Importantly, the interaction between primary afferent nociceptors (associated with the DRG) and sympathetic efferents during inflammation appears to be increased for intact nociceptors with axons travelling in damaged nerve (Sato & Perl 1991). Conversely, the sympathetic postganglionic neurones also release mediators, which decrease plasma extravasation, including neuropeptide Y and noradrenaline (Green et al. 1991; 1992). Apart from modulating plasma extravasation these substances may also interact with endothelial relaxing factor (Greenberg et al. 1991) and platelet-activating factor (Heller et al. 1994) in the blood vessels. Significantly, agents that enhance synovial plasma extravasation have been demonstrated to decrease tissue injury during inflammation (Coderre et al. 1991). The mechanisms by which sympathetic nerves decrease tissue injury are unclear. However, an increased plasma extravasation would be expected to reduce the concentration of inflammatory substances through the facilitation of venous drainage thereby improving healing (Heller et al. 1994) at the terminals of the SNV nerve. These animal investigations suggest that in addition to non-invasive autonomic testing, the motivational-affective responses need to be monitored using psychometric pain questionnaires.
DURATION OF EFFICACY: THE 'SILENCING' OF ECTOPIC IMPULSE GENERATORS COULD LEAD TO A PROLONGED EFFECT SIMILAR TO LOCAL ANAESTHETICS.
The relief of pressure from extraneural inflammatory compromise at SNV nerve receptor sites surrounding the DRG could 'silence' ectopic impulse discharges. Ideally, this 'silencing' would last for a similar duration to that demonstrated by local anaesthetics. Local anaesthetics 'silence' the neurones at the site of ectopic impulse generation for a period outlasting the pharmacological effect of the local anaesthetic (Devor et al. 1992). It has been hypothesised that any silencing of ectopic discharges should allow the autoinhibitory interneurones of the spinal cord to recover from the neurotoxic effects of increased large diameter afferent bombardment (Sugimoto et al. 1990; Dubner 1991). Alternatively, this 'silencing' may provide the sensory-discriminative pathway an opportunity to activate powerful descending inhibition of pain and inflammation. A reduction in ectopic discharge has been shown in cats when the compression stimulus was removed (Howe et al. 1977). Thus, if a technique reduces endoneurial oedema by assisting in the removal of extraneural inflammatory exudate from around the DRG and SNV nerve, then this may explain any normalisation of neurological signs and symptoms for a duration outlasting the period of the technique. Importantly, the demonstration of such temporal responses, once the biomechanical stimuli of our techniques has been removed, would highlight the overwhelming influence of the neurophysiological processes in healing.
CONCLUSION
Reduced mechanical irritation of the DRG in the IVF may be responsible for the immediate and long lasting effects of the appropriate treatment for acute radicular pain, in some people. Consequently, reduced ectopic impulse generation and enhanced modulation of pain and inflammation should be accompanied by the normalisation of signs and symptoms. Sensory-discriminative and motivational-affective nervous system responses are likely mechanisms required for the prolonged normalisation of signs and symptoms. Clearly, future investigations into the efficacy of manual therapy, requires the incorporation of higher centre processing into the methodology. Vascular changes as a result of inflammation are probably modulated by the sympathetic nervous system (SNS). Improved blood flow allows the restoration of the homeostatic function of the DRG. Additionally, the modulation of the excitability of sensory nerve terminals, by the DRG, involves its interaction with the SNS. Enhanced modulation of prostaglandin activity through the interaction of the DRG and SNS with the cytokine-immune system at the sites of innervation of the SNV nerve may restore nerve conduction. The two-threshold hypothesis for the dose of traction could represent a novel experimental method, as it is unlikely that a person can guess the threshold of their normalisation of signs and symptoms. A promising investigative model, using the dose of traction, psychometric analysis, computer modelling, in addition to diagnostic imaging, represents a potential methodology for unravelling the mysteries of radicular pain. The effect of appropriate early intervention to the incidence of chronicity requires investigation, since the validity and precise incidence of the normalisation of signs and symptoms during the treatment of acute radicular pain has not been clearly established. Hereby, charges of physiotherapy induced conviction of disease leading to chronicity can be addressed.
all intellectual property rights should be observed; written predominantly in early 1995 as part of my Masters in Applied Science (Manipulative Physiotherapy)
https://www.sciencedirect.com/science/article/abs/pii/S1356689X00902352
uploaded by Martin Krause 2000
Descending modulation of pain hypothesis vindicated by recent research:
Skyba DA, et al (2003) Joint manipulation reduces hyperalgesia by activation of monoamine receptors but not opioid or GABA receptors in the spinal cord. Pain, 106, 159-168
Ren & Dubner (2002). Descending Modulation of Pain: Pain, 100, 1-6
see also
Tumor necrosis factor α and interleukin-1β stimulate the expression of cyclooxygenase II but do not alter prostaglandin E2 receptor mRNA levels in cultured dorsal root ganglia cells
Fehrenbacher JC, et al (Link to article at on-line Pain journal at Elsevier.com)
Abstract
Tumor necrosis factor α (TNFα) and interleukin 1β (IL-1β) are pro-inflammatory cytokines capable of altering the sensitivity of sensory neurons. Because sensitization elicited by IL-1β and TNFα is blocked by inhibition of the inducible enzyme, cyclooxygenase-II (COX-2), we examined whether these cytokines could increase COX-2 expression in dorsal root ganglion (DRG) cultures. Treatment of cell cultures with either IL-1β or TNFα increases immunoreactive COX-2, as measured by immunoblotting, in a time- and concentration-dependent manner. A 24-h pretreatment with 10 ng/ml IL-1β or 50 ng/ml TNFα augmented COX-2 expression 50- and 8-fold over basal levels, respectively. Immunohistochemistry established the presence of COX-2-like immunoreactivity in both neuronal and non-neuronal cells in culture. The addition of IL-1 receptor antagonist blocked the induction of COX-2 expression by IL-1β, but did not alter TNFα-stimulated increases in COX-2, indicating that the mechanism of TNFα is not limited to increasing the expression of IL-1β. The basal and TNFα-induced expression of COX-2 was not dependent on the presence of NGF in the growth media. IL-1β and TNFα treatment for 24 h enhanced prostaglandin E2 (PGE2) production 2–4-fold, which was blocked by pretreatment with the COX-2 inhibitor, NS-398. Exposing cultures to PGE2, IL-1β, or TNFα for 24 h did not alter PGE2 receptor (EP) mRNA levels. These results indicate that TNFα and IL-1β induce the functional expression of COX-2 but not EP receptors in DRG cells in culture and suggest that cytokine-induced sensitization of sensory neurons is secondary to prostaglandin production and not alterations in EP receptors.
Late in 2007, DeLeo, Sorkin & Watkins in their IASP publication Immune and glial regulation of pain devoted 5 chapters (of 23) to the DRG. Chapter 9 described DRG signaling and erythropoietin as a protective agent against neuropathic pain development (Campana, WM), chapter 10 cited the recognition that DRG satellite cells and trafficking leukocytes into the DRG may directly affect primary afferent signaling which enhances the complexity of glial - immune reactions within the CNS (McLachlan E). Chapter 21 described the ischaemic compromise due to the metabolic demands of immune - inflammatory processes in the DRG, as well as describing both pro-inflammatory (IL-1, IL-6, TNF-alpha) and anti-inflammatory (IL-10) cytokines found in the Nucleus Pulposus of the disk.
McLachlan EM, Hu P (2007). Inflammation of DRG: Satellite cell activation and immune cell recruitment after nerve injury. In : Immune and Glial Regulation of Pain Ed DeLeo JA, Sorkin LS, Watkins LR. IASP Press, Seattle. Ch 10
- Neuropathic pain generally developes following lesions of the blood-nerve barrier. Neurogenic inflammation as a result of mechanical irritation leading to chemical irritants and oedema can precipitate the conditions required for the development of neuropathic pain. Retrograde axonal signalling from nociceptors that surround the DRG itself can propagate inflammatory reactions around the somata of motor, sympathetic and sensory neurones triggering the release of chemokines from the glia of satellite cells within the DRG and astrocytes in the ventral horn.
- In contrast to the CNS, the blood-nerve barrier around the DRG is very permeable thus allowing the the neurones to be exposed to circulating proteins (and potentially the extruded disk material such as the nucleus pulposus (NP) - my thoughts).
- Transection or ligation of the L5 spinal nerve is followed by degeneration of axons in the distal branches of the sciatic nerve. Interestingly, the L4 DRG shows mild but distinct inflammatory responses with invasion of macrophages and lymphocytes. This finding indicates that DRG inflammation can be triggered by signals independent of axotomy of it's sensory neurones.
- The chronic constriction injury model using loose ligatures around the sciatic nerve there is recruitment of alpha-beat T-lymphocytes into the DRG and the spinal cord. Amost all are CD8+ T cells. Unless T cells and macrophages in the subarachnoid angle are intravascular, penetration of the capsule is likely to require the upregulation of chondroitin sulphate proteoglycan degrading enzymes such as metalloproteinases, as has been shown in sympathetic ganglia (Leone et al 2005).
- The most likely effect of inflammation within the DRG is to reduce discharge threshold of injured and non-injured neurones that project centrally in pain pathways. Another factor that may raise neuronal excitability and initiate discharge is the relative ischaemia resulting from the higher metabolic demands of inflammation.
Karppinen J (2007). New perspectives on Sciatica. In : Immune and Glial Regulation of Pain Ed DeLeo JA, Sorkin LS, Watkins LR. IASP Press, Seattle. Ch 21
- A sharp 40-98% decrease in intraradicular blood flow in the L5 and L4 was elicited by an intraoperative straight leg raising test at the angle which produced symptoms of sciatica. Removal of adhesions normalised blood flow highlighting the importance of mechanical compression in the induction of ischaemia.
- However, inflammation may induce ischaemia through increased endoneurial pressure from capillary leakage similar to a 'compartment syndrome' of the DRG.
- In contrast to nerve roots, the DRG are very sensitive to mechanical compression.
- Both mechanical and chemical irritation produce more severe histological damage to the nerve roots than either factor alone.
- Hypoxia-inducible factor (HIF), a transcription factor that responds to low oxygen levels, probably triggers mitogen-activated protein kinase (MAPK) expression and erythropoietin synthesis.
- Tumor necrosis factor alpha is crucial in MAPK activation
- Exposure of the DRG to IL-1beta, TNF-alpha, and IL-6 increased mechanosensitivity of DRG and it's receptive fields
- Antereograde activation of spinal cord glial cells (astrocytes and microglia) by cytokines can result in extra-territorial pain and mirror image pain
- Herniated disk material contains pro-inflammatory as well as anti-inflammatory (IL-10) cytokines.
See the following link for a greater explanation of the neuro-immune-inflammatory cascade as it relates to exercise, muscle protein, apoptosis and cognitive behavioural therapy.
Immune System and Musculoskeletal Dysfunction
References
Adams, M.A., Dolan, P.& Hutton, W.C. (1986). The stages of disc degeneration as revealed by discogram. Journal of Bone and Joint Surgery 68B, 36.
Ahmed, M., Bjurholm, A., Kreicbergs, A.& Schultzberg, M. (1993). Sensory and autonomic innervation of the facet joint in the rat lumbar spine. Spine 18(14), 2121 to 2126.
Alkon, D.L.& Rasmussen, H.A. (1988). A spatial-temporal model of cell activation. Science 239, 998 to 1005.
Attal, N., Filliatreau, G., Perrot, S., Jazat, F., Di Giamberardino, L.& Guilbaud, G. (1994). Behavioural pain-related disorders and contribution of the saphenous nerve in crush and chronic constriction injury of the rat sciatic nerve. Pain 59, 301 to 312.
Badalemente, M.A., Dee, R., Ghillani, R., Chien, P-F. & Daniels, K. (1987). Mechanical stimulation of dorsal root ganglia induces increased production of substance P : A mechanism for pain following nerve root compromise? Spine 12, 552 to 555.
Barasi, S.& Lynn, B. (1986). Effects of sympathetic stimulation on mechanoreceptive and nociceptive afferent units from the rabbit pinna. Brain Research 378, 21 to 27.
Barker, J.N., Mitra, R.S., Griffiths, C.E., Dixit, V.M.& Nicholoff, B.J. (1991). Keratinocytes as initiators of inflammation. Lancet 337, 211 to 214.
Barrows, H.S., Tamblyn, R.N., (1980). Problem-based learning: an approach o medical education. Springer, New York.
Blottner, D.& Baumgarten, H.G. (1994). Neurotrophy and regeneration in vivo. Acta Anatomica 150, 235 to 245.
Bogduk, N. (1993). The anatomy and physiology of nociception. In : Crosbie J.& McConnell, J.(Eds.) (1993). Key Issues in Musculoskeletal Physiotherapy(Ch.3). Oxford : Butterworth-Heinemann Ltd.
Butler, D.S., (1991). Mobilisation of the Nervous System. Churchill Livingstone : Melbourne.
Chatani, K., Kawakami, M., Weinstein, J.N., Meller, S.T.& Gebhart, G.F. (1995). Characterization of thermal hyperalgesia, c-fos expression, and alterations in neuropeptides after mechanical irritation of the dorsal root ganglion. Spine 20(3), 277 to 290.
Coderre, T.J., Basbaum, A.I.& Levine, J.D. (1989). Neural control of vascular permeability : interactions between primary afferents, as cells, and sympathetic efferents. Journal of Neurophysiology 62, 48 to 58
Coderre, T.J., Chan, A.K., Helms, C.& Levine, J.D. (1991). Increasing sympathetic nerve terminal-dependent plasma extravasation correlates with decreased arthritic joint injury in rats. Neuroscience 40, 185 to 189.
Coghill, R.C., Mayer, D.J., Price, D.D., (1993). Spinal cord coding of pain : The role of spatial recruitment and discharge frequency in nociception. Pain, 53, 295 to 309.
Cohen, M.L., (1995). The clinical challenge of secondary hyperalgesia. Moving in on Pain (Abstracts). Adelaide, Australia.
Cohen, M.L., Quintner, J.L., (1993). Fibromyalgia syndrome, a problem of tautology. Lancet, 342, 906-909.
Collingride, G.L.& Singer, W. (1990). Excitatory amino acid receptors and synaptic plasticity. Trends in Pharmacological Science 11, 290 to 296.
Cornefjord, M., Takahashi, K., Matsui, H., Olmarker, K., Holm, S.& Rydevik, B. (1992). Impairment of nutritional transport at double level cauda equina compression: An experimental study. Neuro Orthopedics 13, 107 to 112.
Dickenson, A.H.& Sullivan, A.F. (1987). Evidence for a role of the NMDA receptor in the frequency dependent potentiation of deep rat dorsal horn nociceptive neurons following C-fibre stimulation. Neuropharmacology 26, 1235 to 1238.
Donnerer, J., Amann, R. & Lembeck, F. (1991). Neurogenic and non-neurogenic inflammation in the rat paw following chemical sympathectomy. Neuroscience 45(3), 761 to 765.
Enwemeka, C.S. & Spielholz, N.I. (1992). Modulation of tendon growth and regeneration by electrical fields and currents. In : Currier, D.P.& Nelson, R.M. (Eds.) (1992). Dynamics of Human Biologic Tissues (ch10). Philadelphia : F.A. Davis Company.
Ferrell, W.R., Wood, L. & Baxendale, R.H. (1988). The effect on acute joint inflammation on flexion reflex excitability in the decerebrate, low-spinal cat. Quarterly Journal Of Experimental Physiology 73, 95 to 102.
Galea, M.P. & Darien-Smith, I. (1995). Voluntary movement and pain : Focussing on action rather than perception. Moving in on Pain. Adelaide.
Gallin, J.I., Goldstein, I.M. & Snyderman, R. (Eds.) (1992). Inflammation : Basic Principles and Clinical Correlates (2nd ed.). New York : Raven Press.
Gogas, K.R., Presley, R.W., Levine, J.D. & Basbaum, A.,I., (1991). The antinociceptive action of supraspinal opioids results from an increase in descending inhibitory control : Correlation of nociceptive behaviour and C-fos expression. Neuroscience 42(3), 617 to 628.
Gracely, R.H., Lynch, S.L. & Bennett, G.,J. (1992). Painful neuropathy : Altered central processing, maintained dynamically by peripheral input. Pain 51, 175 to 194.
Greenbag, P.E., Brown, M.D., Pallares, V.S., Tompkins, J.S. & Mann, N.,H., (1988). Epidural anesthesia for lumbar spine surgery. Journal of Spinal Disorders 1, 139 to 143.
Gonzales, R., Goldyne, M.E., Taiwo, Y.O. & Levine, J.D. (1989). Production of hyperalgesic prostaglandins by sympathetic postganglionic neurons. Journal of Neurochemistry 53, 1595 to 1598.
Gonzales, R., Sherbourne, C.D., Goldyne, M.E. & Levine, J.D., (1991). Noradrenaline-induced prostaglandin production by sympathetic postganglionic neurons is mediated by alpha-2-adrenergic receptors. Journal of Neurochemistry 57, 1145 to 1150.
Green, P.G., Basbaum, A.I., Helms, C. & Levine, J.D. (1991). Purinergic regulation of bradykinin-induced plasma extravasation and adjuvant-induced arthritis in the rat. Proceedings of the National Academy of Science, U.S.A. 88, 4162 to 4165.
Green, P.G., Luo, J., Heller, P.H. & Levine, J.D. (1992). Modulation of bradykinin-induced plasma extravasation in the rat knee joint by sympathetic co-transmitters. Neuroscience 52, 451 to 458.
Groen, G.J., Balget, B. & Drukker, J. (1988). The innervation of the spinal dura mater: anatomy and clinical considerations. Acta Neurochirurgica 92, 39 to 46.
Groenblad, M., Weinstein, J.N. & Santavirta, S. (1991). Immunohistochemical observation on spinal tissue innervation. Acta Orthopaedic Scandinavia 62(6), 614 to 622.
Groenblad, M., Virri, J., Tolonen, J., Seitsalo, S., Kaeaepae, E., Kankare, J., Myllynen, P. & Karaharju, E. (1994). A controlled immunohistochemical study of inflammatory cells in disc herniation tissue. Spine 19(24), 2744 to 2751.
Handwerker, H.O., Forster, C. & Kirchhoff, C., (1991). Discharge patterns of human C-fibres induced by itching and burning stimuli. Journal of Neurophysiology 66, 307 to 317.
Harvey, G.K., Toyka, K.V. & Hartung, H.-P. (1994). Effects of mast cell degranulation on blood-nerve barrier permeability and nerve conduction in vivo. Journal of the Neurological Sciences 125, 102 to 109.
Heller, P.H., Green, P.G., Tanner, K.D., Miao, F.J.-P. & Levine, J.D. (1994). Peripheral neural contributions to inflammation. Progress in Pain Management (1st ed.)(pp31 to 42). Seattle : IASP Press.
Hodges, P., Richardson, C., (1996). Inefficient muscular stabilisation of the lumbar spine associated with low back pain : A motor control evaluation of transverse abdominis. Spine, 21, 2640 to 2650.
Hodges, P., Richardson, C., Jull, G., (1996). Evaluation of the relationship between laboratory and clinical tests of transverse abdominis function. Physiotherapy Research International, 1, 30 to 40.
Hu, S. & Zhu, J. (1989). Sympathetic facilitation of sustained discharges of polymodal nociceptors. Pain 38, 85 to 90.
Hsieh, J-C., Stahle-Backdahl, M., Hagermark, O., Stone-Elander, S., Rosenquist, G., Ingvar, M., (1995). Traumatic nociceptive pain activates the hypothalamus and the periaqueductal gray: a positron emission tomography study. Pain, 64, 303 to 314.
Issekutz, T.B. (1992). Inhibition of lymphocyte endothelial adhesion and in vivo lymphocyte migration to cutaneous inflammation by TA-3, a new monoclonal antibody to rat LFA-1. Journal of Immunology 149, 3392 to 3402.
Jaenig, W. (1985). Organization of the lumbar sympathetic outflow to skeletal muscle and skin of the cat hind limb and tail. Review of Physiology, Biochemistry, Pharmacology 102, 119 to 213.
Jaenig, W. & Koltzenberg, M. (1991). Receptive properties of pial afferents. Pain 45, 77 to 85.
Jones, M., (1995). Clinical Reasoning and Pain. Manual Therapy, 1, 17 to 24.
Jull, G., Zito, G., Trott, P., Potter, H., Shirley, D., Richardson, C., (1997). Inter-examiner reliability to detect painful upper cervical joint dysfunction. Australian Journal of Physiotherapy, 43, 2, 125 to 129.
Kalso, E.A., Sullivan, A.F., McQuay, H.J., Dickenson, A.H., Roques, B.P., (1993). Cross-tolerance between Mu Opioid and alpha-2 Adrenergic receptors, but not between Mu and Delta receptors in the spinal cord of the rat. The Journal of Pharmacology and Experimental Therapeutics, 265 (2), 551 to 558.
Kambin, P., Abda, S. & Kurpici, F. (1980). Intradiskal pressure and volume recording : Evaluation of normal and abnormal intervertebral disks. Clinical Orthopedics 146, 140.
Kawakami, M., Weinstein, J.N., Chatani, K.-I., Spratt, K.F., Meller, S.T. & Gebhart, G.F. (1994a). Experimental lumbar radiculopathy : Behavioural and histologic changes in a model of radicular pain after spinal nerve root irritation with chromic gut ligatures in the rat. Spine 19(16), 1795 to 1802.
Kawakami, M., Weinstein, J.N., Spratt, K.F., Chatani, K-I., Traub, R.J., Meller, S.T. & Gebhart, G.F. (1994b). Experimental lumbar radiculopathy : Immunohistochemical and quantitative demonstrations of pain induced by lumbar nerve root irritation of the rat. Spine 19(16), 1780-1794.
Kobayashi, S., Yoshizawa, H., Hachiya, Y., Ukai, T. & Morita, T. (1993). Vasogenic edema induced by compression injury to the spinal nerve root: Distribution of intravenously injected protein tracers and Gadolinium-Enhanced Magnetic Resonance Imaging. Spine 18(11), 1410 to 1424.
Koltzenburg, M., Kees, S., Budweiser, S., Ochs, G. & Toyka, K.V. (1994). The properties of unmyelinated nociceptive afferents change in a painful chronic constriction neuropathy. In : Gebhart, G.F., Hammond, D.L. & Jensen, T. S. (Eds.) (1994). Proceedings of the 7th World Congress on Pain : Progress in Pain and Management (2nd ed.) (Ch.35). Seattle : IASP Press.
Korkala, O., Gronblad, M., Liesi, P. & Karaharju, E. (1985). Immunohistochemical demonstration of nociceptors in the ligamentous structures of the lumbar spine. Spine 10, 156 to 157.
Kuslich, S.D., Ulstrom, C.L. & Michael, C.J. (1991). The tissue origin of low back pain and sciatica: A report of pain response to tissue stimulation during operation on the lumbar spine using local anaesthesia. Orthopedic Clinics North America 22, 181 to 187.
Laird, J.M.A. & Bennett, G.J. (1993). An electrophysiological study of dorsal horn neurons in the spinal cord of rats with an experimental peripheral neuropathy. Journal of Neurophysiology 69, 2072 to 2085.
Laird, J.M.A. & Cervero, F. (1990). Tonic descending infuences on receptive-field properties of nociceptive dorsal horn neurons in sacral spinal cord of rat. Journal of Neurophysiology 63(5), 1022 to 1032.
LaMotte, R.H., Shane, C.N., Simone, D.A. & Tsai, E.F.P. (1991). Neurogenic hyperalgesia : Psychophysical studies of underlying mechanisms. Journal of Neurophysiology, 66, 190 to 211.
Levine, J.D., Dardick, S.J., Roizen, M.F., Helms, C. & Basbaum, A.I. (1986). The contribution of sensory afferents and sympathetic efferents to joint injury in experimental arthritis. Journal of Neuroscience 6, 3923 to 3929.
Levine, J.D., Goldstine, J., Mayes, M., Moskowitz, M.A. & Basbaum, A.I. (1986). The neurotoxic effect of gold sodium thiomalate on the peripheral nerves of the rat. Arthritis and Rheumatism 29, 897 to 901.
Levine, J.D., Taiwo, Y.O., Collins, S.D. & Tam, J.K. (1986a). Noradrenaline hyperalgesia is mediated through interaction with sympathetic postganglionic neurone terminals rather than activation of primary afferent nociceptors. Nature 323, 158 to 160.
Lotz, M., Vaughn, J.H. & Carson, D. (1988). Effect of neuropeptides on production of inflammatory cytokines by human monocytes. Science 241, 1218 to 1221.
Lovick, T.A., (1991). Interactions between descending pathways from the dorsal and ventrolateral periaquaductal gray matter in the rat. In ; Depaulis, A., Bandler, R.,(eds). The Midbrain Periaqueductal Gray Matter. Plenium Press, New York, 101 to 120.
Lima, D., Esteves, F. & Coimbra, A., (1994). C-fos activation by noxious input of spinal neurons projecting to the nucleus of the tractus solitarius in the rat. In : Gebhart, G.F., Hammond, D.L. & Jensen, T.S. (Eds.) (1994). Proceedings of the 7th World Congress on Pain : Progress in Pain and Management (2nd ed.) (Ch.30). Seattle : IASP Press.
Liu, J., Roughley, P.J. & Mort, J.S. (1991). Identification of human intervertebral disc stromelysin and its involvement in matrix degeneration. Journal of Orthopedic Research 9, 568 to 575.
Lundborg, G., (1988). Nerve Injury and Repair. Edinburgh : Churchill Livingstone
MacMillan, J., Schaffer, J.L. & Kambin, P. (1991). Routes and incidence of communication of lumbar discs with surrounding neural structures. Spine 16, 2, 167 to 171.
Magal, E.L. (1990). Gangliosides prevent ischemia-induced down-regulation of protein kinase C in fetal rat brain. Journal of Neurochemistry 55, 2126 to 2131.
Maitland, G.D. (Ed.) (1986). Vertebral Manipulation (5th ed.). London : Butterworths.
Maitland, G.,D., (Ed) (1991). Peripheral Manipulation. London : Butterworths.
Mao, J., Price, D.D., Coghill, R.C., Mayer, D.J. & Hayes, R.L. (1992). Spatial patterns of spinal cord [14C]-2-deoxyglucose metabolic activity in a rat model of painful peripheral mononeuropathy. Pain 50, 89 to 100.
Markowitz, S., Saito, K., Buzzi, M.G. & Moskowitz, M.A. (1989). The development of neurogenic plasma extravasation in the rat dura mater does not depend upon the degranulation of mast cells. Brain Research 477, 157 to 165.
Matsui, H., Olmarker, K., Cornefjord, M., Takahashi, K. & Rydevik, B. (1992). Local electrophysiological stimulation in experimental double level cauda equina compression. Spine, 17(9), 1075 to 1078.
Maixner, W., Gracely, R.H., Zuniga, J.R., Humphrey, C.B & Bloodworth, G.R. (1990). Cardiovascular and sensory responses to forearm ischemia and dynamic hand exercise. American Journal of Physiology 259, R1156 to R1163.
McKenzie, R.C. & Sauder, D.N. (1990). The role of keratinocyte cytokines in inflammation and immunity. Journal of Investigative Dermatology 95, S105 to 107.
Morton, C.R., Siegel, J., Xiao, H.-M., Zimmermann, M., (1997). Modulation of cutaneous nociceptor activity by electrical stimulation in the brain stem does not inhibit the nociceptive excitation of dorsal horn neurons. Pain, 71, 65 to 70.
Morgan, M.M., Sohn, J.-H., Lohof, A.M. Ben-Eliyahu, S. & Liebeskind, J.C. (1989). Characterization of stimulation-produced analgesia from the nucleus tractus solitarius in the rat. Brain Research 486, 175 to 180.
Nakagawa, I., Omote, K., Kitahata, L.M., Collins, J.G. & Murata, K. (1990). Serotonergic mediation of spinal analgesia and its interaction with noradrenergic systems. Anesthesiology 73, 474 to 478.
Nishizuka, Y. (1989). The family of protein kinase C for signal transduction. JAMA 262, 1826 to 1833.
Ochoa, J.L. & Yarnitsky, D. (1993). Mechanical hyperalgesia in neuropathic pain patients : Dynamic and static subtypes. Annals of Neurology 33, 465 to 472.
Olmarker, K., Rydevik, B., Holm, S. & Bagge, U. (1989). Effects of experimental, graded compression on blood flow in spinal nerve roots. A vital microscope study on the porcine cauda equina. Journal of Orthopedic Research 7, 817 to 823.
Olmarker, K., Rydevik, B. & Nordborg, C. (1993). Autologous Nucleus Pulposus induces neurophysiological and histological changes in porcine cauda equina nerve roots. Spine 18(11), 1425 to 1432.
Petersen, N.,P., Vicenzino, B., Wright, A., (1993). The effects of a cervical mobilisation technique on sympathetic outflow to the upper limb in normal subjects. Physiotherapy Theory and Practice, 9, 149 to 156.
O'Sullivan, P., Twomey, L., Allison, G., Sinclair, J., Miller, K., Knox, J., (1997). Altered patterns of abdominal muscle activation in patients with chronic low back pain. Australian Journal of Physiotherapy, 43, 91 to 98.
Post, C., Minor, B.G., Davies, M. & Archer, T. (1986). Analgesia induced by 5-hydroxytryptamine-depletion in rats. Brain Research 363, 18 to 27.
Price, D.D., Long, S. & Huitt, C. (1992). Sensory testing of pathophysiological mechanisms of pain in patients with reflex sympathetic dystrophy. Pain 49, 163 to 173.
Price, D.D., Mao, J. & Mayer, D.J. (1994). Central neural mechanisms of normal and abnormal pain states. In Fields, H.L. & Liebeskind, J.C. (Eds.)(1994). Progress in Pain Research and Management(1st ed.)(pp61 to 84). Seattle : IASP Press.
Proudfit, H.K. (1992). The behavioural pharmacology of the noradrenergic descending system. In : Besson, J.M. & Guilbaud, G. (Eds.)(1992). Towards the use of Noradrenergic Agonists for the Treatment of Pain(1st ed.). Amsterdam : Elsevier Science Publishers B.V.
Quintner, J.L., Cohen, M.L., (1994). Referred pain of peripheral nerve origin : an alternative to the 'myofascial pain construct'. Clinical Journal of Pain, 10, 243 to 251.
Raja, S.N., Meyer, R.A. & Campbell, J.N. (1988). Peripheral mechanisms of somatic pain. Anesthesiology 68, 571 to 590.
Rees, H., Sluka, K.A., Westlund, K.N. & Willis, W.D. (1994). Do dorsal root reflexes augment peripheral inflammation ? NeuroReport 5, 821 to 824.
Ren, K., Randich, A. & Gebhart, G.F. (1990). Modulation of spinal nociceptive transmission from nuclei tractus solitarii : A relay for effects of vagal afferent stimulation. Journal of Neurophysiology 63(5), 971-986.
Roberts, W.J. & Elardo, S.M. (1985). Sympathetic activation of unmyelinated mechanoceptors in cat skin. Brain Research 339, 123 to 125.
Rothwell, N.J. & Hopkins, S.J. (1995). Cytokines and the nervous system II : actions and mechanisms of action. Trends in Neuroscience 18, 130 to 136.
Rydevik, B.L., Brown, M.D. & Lundborg, G. (1984). Pathoanatomy and pathophysiology of nerve root compression. Spine 9, 7 to 15.
Rydevik, B.L., Myers, R.R. & Powell, H.C. (1989). Pressure increase in the dorsal root ganglion following mechanical compression: Closed compartment syndrome in nerve roots. Spine 14(6), 574 to 576.
Sandkuehler, J., Eblien-Zajjur, A., Fu, Q.-G. & Forster, C. (1995). Differential effects of spinalization on discharge patterns and discharge rates of simultaneously recorded nociceptive and non-nociceptive spinal dorsal horn neurons. Pain 60, 55 to 65.
Sanjue, H. & Jun, Z. (1989). Sympathetic facilitation of sustained discharges of polymodal nociceptors. Pain 38, 85 to 90.
Schmidt, R.F. (1990). Experimental arthritis. Pain(supp) 5, S215.
Schmidt, R.F., Schaible, H.-G., Messlinger, K., Heppelmann, B., Hanesch, U. & Pawlak, M. (1994). Silent and active nociceptors : Structure, functions, and clinical implications. In : Gebhart, G.F., Hammond, D.L. & Jensen, T. S. (Eds.) (1994). Proceedings of the 7th World Congress on Pain : Progress in Pain and Management (Ch.16) (2nd ed.). Seattle : IASP Press.
Shindo, K., Tsunoda, S-T.& Shiozawa, Z. (1994). Muscle spasm induced sympathetic reflex bursts on microneurography in a case with pontine demyelination. Clinical Autonomic Research 4, 299 to 302.
Schomburg, E.,D. & Steffens, H. (1992). On the spinal motor function of nociceptive afferents and enkephalins. In : Jami, L., Pierrot-Deseilligny, E. & Zytnicki, D. (Eds.)(1992). Muscle Afferents and Spinal Control of Movement(pp.395-400)(1st ed.). Oxford : Pergamon Press.
Suval, W.D., Duran, W.N., Boric, M.P., Hobson, R.W., Berendsen, P.B. & Ritter, A.B. (1987). Microvascular transport and endothelial cell alterations preceding skeletal muscle damage in ischemia and reperfusion injury. The American Journal of Surgery 154, 211 to 218.
Taiwo, Y.O. & Levine, J.D. (1989). Prostaglandin effects after elimination of indirect hyperalgesic mechanisms in the skin of the rat. Brain Research 492, 397 to 399.
Takahashi, K., Olmarker, K., Holm, S., Porter, R.W. & Rydevik, B. (1993). Double level cauda equina compression. An experimental study with continuous monitoring of intraneural blood flow in the porcine cauda equina. Journal of Orthopedic Research 11(1), 104 to 109.
Thompson, S.W.N. & Woolf, C.J. (1991). Primary afferent-evoked prolonged potentials in the spinal cord and their central summation : Role of the NMDA receptor. In : Bond, M.R., Charlton, J.E. & Woolf, C.J. (Eds). Proceedings of the VIth World Congress on Pain(pp291-298). Amsterdam : Elsevier
Tillman, L.J. & Cummings, G.S. (1992). Biologic mechanisms of connective tissue mutability. In : Currier, D.P. & Nelson, R.M. (Eds.) (1992). Dynamics of Human Biologic Tissues (pp1-44). Philadelphia : F.A. Davis Company.
Torebjoerk, E. (1994). Nociceptor dynamics in humans. In : Gebhart, G.F., Hammond, D.L. & Jensen, T. S. (Eds.) (1994). Proceedings of the 7th World Congress on Pain : Progress in Pain and Management (Ch.19) (2nd ed.). Seattle : IASP Press.
Troisier, O. & Cypel, D. (1986). Discography: An element of decision. Clinical Orthopedics 206, 70.
Urban, L. & Randic, M. (1984). Slow excitatory transmission in rat dorsal horn : Possible mediation by peptides. Brain Research 290, 336 to 341.
Vaccarino, F., Guidotti, A. & Costa, E. (1987). Ganglioside inhibition of glutamate-mediated protein kinase C translocation in primary cultures of cerebellar neurons. Proceedings of the National Academy of Science, U.S.A. 34, 8707.
Wall, P.D. (1995). Treatment of pain. Moving in on Pain. Adelaide.
Wall, P.D. & Devor, M. (1983). Sensory afferent impulse originate from dorsal root ganglia as well as from the periphery in normal and nerve injured rats. Pain 17, 321-339.
Wall, P.D. & Melzak, R. (1989) (Eds.). Textbook of Pain, (2nd. ed.). Edinburgh : Churchill Livingstone.
Weinstein, J.N., Claverie, W. & Gibson, S. (1988). The pain of discography. Spine 13(12), 1344 to 1348.
Williams, T.J. & Hellewell, P.G. (1992). Endothelial cell biology. Adhesion molecules involved in the microvascular inflammatory response. American Review of Respiratory Disease 146, S45 to 50.
Wiltse, L.L., Fonseca, A.S., Amster, J., Dimartino, P. & Ravessoud, F.A. (1993). Relationship of the dura, Hofmann's ligaments, Batson's plexus, and a fibrovascular membrane lying on the posterior surface of the vertebral bodies and attaching to the deep layer of the posterior longitudinal ligament: An anatomical, radiological, and clinical study. Spine 18(8), 1030 to 1043.
Woolf, C.J. (1983). Evidence for a central component of post-injury pain hypersensitivity. Nature 306, 686 to 688.
Woolf, C.J. (1984). Long-term alterations in the excitability of the flexion reflex produced by peripheral tissue injury in the chronic decerebrate rat. Pain 18, 325 to 343.
Woolf, C.J. & McMahon, S.B. (1985). Injury-induced plasticity of the flexor reflex in chronic decerebrate rats. Neuroscience 16, 395-404.
Woolf, C.J., Shortland, P. & Sivilotti, L.G. (1994). Sensitization of high mechanothreshold superficial dorsal horn and flexor motor neurones following chemosensitive primary afferent activation. Pain 58, 141 to 155.
Woolf, C.J. & Swett, J.E. (1984). The cutaneous contribution to the hamstring flexor reflex in the rat : an electrophysiological and anatomical study. Brain Research 303, 299 to 312.
Woolf, C.J. & Wall, P.D. (1986). Relative effectiveness of C primary afferent fibres in evoking a prolonged facilitation of the flexor reflex in the rat. The Journal of Neuroscience 6, 1433 to 1442.
Wright, A., Vicenzino, B., (1995). Cervical mobilisation techniques, sympathetic nervous system effects and their relationship to analgesia. In : Schacklock, M.,O., (ed.). (1995). Moving in on Pain, Butterworth-Heineman, 164 to 173.
Xavier, A.V., Farrell, C.E., McDanal, J. & Kissin, I. (1990). Does antidromic activation of nociceptors play a role in sciatic radicular pain? Pain 40, 77 to 79.
Zochodne, D.W. (1993). Epineural peptides : A role in neuropathic pain? Canadian Journal of Neurological Sciences 20(1), 69 to 72.
Originally conceived : January - June 1995
Presented at IFOMT and WCPT in Yokohama, Japan - key note address
Published : Manual Therapy 2000
Last update : 7 March 2022
 What We do
What We do What We Treat
What We Treat



















































































































