



Back, Pelvic Girdle and Hip Pain
by Martin Krause
B.Appl.Sci. (Physiotherapy); M.Appl.Sci (Manipulative Physiotherapy), Post Grad Dip Hlth Sc (Exercise and Sports), Post Grad Cert Hlth Sc (Education)
At Back in Business Physiotherapy, we view the pelvis and spine as sitting in a sling of muscles, like a hammock evenly balanced with tension to allow multiple directions of movement without compromising it's stability. Hence, we use a comprehensive analysis with muscle energy techniques, movement analysis, joint mobilisations, soft tissue manipulation and taping to optimise home and gym based exercise regimes. Please read on for more details
List of Contents
Introduction
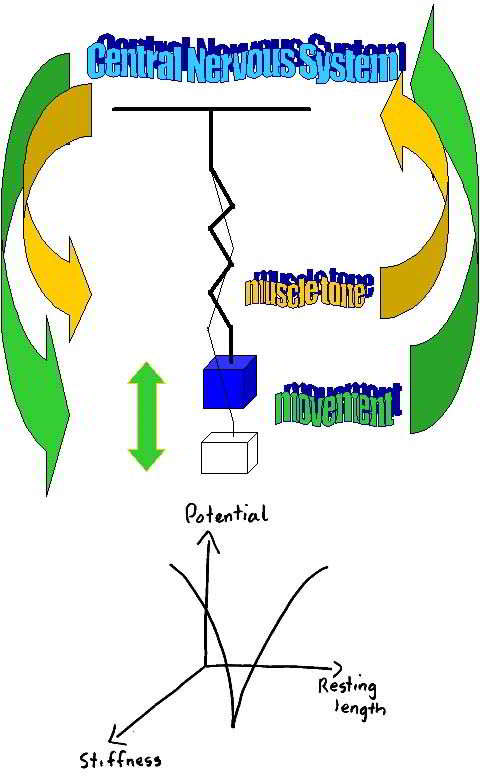
Pelvic girdle and low back pain have fallen under the diagnostic umbrella of non-specific low back pain (NSLBP). Consequently, a misconception that any exercise is good exercise was created. It is true that low back pain can have it's etiology in pelvic girdle mal-alignment, and similarly low back pain with neural irritation can lead to inco-ordination of muscles causing pelvic mal-alignment. However, clinically there appears to be very little non-specific about such problems. Traditionally, manual therapists have viewed impairment as loss of range of motion and/or perceived stiffness on joint mobilization. However, when considering low back pain and pelvic girdle dysfunction, the effects of muscular force transduction are becoming more evident as being an important impairment variable. The clinician needs to be aware of Newton's third law of 'action-reaction', the effects of inverse dynamics and the desire for symmetrical and appropriately timed force dissipation ('damping' and 'propagation') by supporting musculature. Sometimes these are referred to as 'neuromuscular vectors'. Essentially, efficiency of movement is the desired outcome of any movement strategy, whereby muscles are considered as a series of slings acting across joints with differing movement functions. Most of us have experienced the stiffness and awkwardness of movement when learning a novel task. Pain and dysfunction and/or inappropriate physiotherapy can result in excessive stiffness, which compromises the 'fluidity' and range of movement. Hence, such stiffness is the result of non-optimal neuro-muscular firing, rather than passive stiffness based on adhesions, scar tissue or degenerative changes. Good clinical assessment with the application of appropriate muscle energy, manual therapy, soft tissue massage and dry needling techniques for reduction of pain and muscle spasms, as well as appropriate exercise prescription for strength, endurance and motor control can be used as a management strategy whilst simultaneously ascertaining the 'cause of the cause' of dysfunction. Therefore, don't just rush into a Swiss Ball regime.
It is important to understand that motor inco-ordination in the pelvic girdle can be the result of peripheral and/or central mechanisms. Peripheral mechanisms include reflexogenic muscle spasms whilst central mechanisms include cortical inhibition of muscles and/or delayed central transmission due to noxious input affecting intra-cortical synergistic control between various cerebral, cerebellar and mid brain regions of the central nervous system (CNS). Altered proprioceptive input can result in an inaccurate 'virtual body concept of self' resulting in inaccurate feedback during the execution of motor tasks. Attention, stress and fear can inpact motor planning through altered perceptions of task demand and the environment where the execution of the task is to take place.

Build strength and flexibility in stages. The deeper the foundations of motor learning the stronger and greater the scope of adaptation during recovery. Remember there are 3 stages of learning, where the first stage is the cognitive stage in which fundamental movement patterns need to be learnt in the most basic positions of neutral. Then comes the associative stage whereby more dynamic activity or prolonged static postures can be practiced before arriving at the autonomous stage of learning (Fits & Possner 1967, Gentile 1972). Activation of low threshold muscles first, small movements and lots of cognitive motor control. Additionally, deactivation of global muscles and improved timing are frequently early priorities. Later goals may include performance enhancement for return to sport, whereby intramuscular and intermuscular control between and deep stabilising and superficial ballistic muscles is trained using functional exercises which may include the Swiss Ball.
Importantly, determine whether the person is inherently a 'floppy', 'stiffy' or 'flippy-floppy'. The goal with stiff people will be to improve range of motion and acquire control of global muscle timing. Hereby, reducing intra-abdominal and intra-discal pressure. The goal with floppy people will be to enhance stability through co-ordination and improved endurance. Hereby, improving cognitive motor control. Don't get trapped by exacerbating a persons condition, who appears to be stiff, yet has an underlying functional instability. Ask them whether they used to be really flexible as a child or prior to the onset of dysfunction. Also screen for trauma which could have resulted in some functional (and even structural) instability such as lumbar - thoracic spine hyper-flexion-extension from a 'whiplash type' injury such as high speed skiing, marshal arts, etc. Ultimate aims will be to improve lumbo-pelvic dynamics by optimising 'form & force closure' around the symphasis pubis & sacro-iliac joints.
Joint Hypermobility Syndrome (JHS)
includes conditions such as Marfan's Syndrome and Ehlers-Danlos Syndrome and Osteogenesis imperfecta. These people are thought to have a higher proportion of type III to type I collagen, where type I collagen exhibits high tensile strength, whilst type III collagen is much more extensible and disorganised and occuring in organs such as the gut, skin and blood vessels. The predominant presenting complaint is widespread pain lasting from day to decades. Additional symptoms associated with joints, such as stiffness, 'feeling like a 90 year old', clicking, clunking, popping, subluxations, dislocations, instability, feeling that the joints are vulnerable, as well as symptoms affecting other tissue such as paraesthesia, tiredness, faintness, feeling unwell and suffering flu-like symptoms. Autonomic nervous system dysfunction in the form of 'dysautonomia' frequently occur. Broad paper like scars appear in the skin where wounds have healed. Other extra-articular manifestations include ocular ptosis, varicose veins, Raynauds phenomenon, neuropathies, tarsal and carpal tunnel syndrome, alterations in neuromuscular reflex action, development motor co-ordination delay (DCD), fibromyalgia, low bone density, anxiety and panic states and depression. Age, sex and gender play a role in presentaton as it appears more common in African and Asian females with a prevalence rate of between 5% and 25% . Despite this relatively high prevalence, JHS continues to be under-recognised, poorly understood and inadequately managed (Simmonds & Kerr, Manual Therapy, 2007, 12, 298-309). These people tend to move fast, rely on inertia for stability, have long muscles creating large degrees of freedom and potential kinetic energy, where they become the ballistic 'floppies', and either highly co-ordinated or clumsy. There deosn't seem to be in my clincial exprience an in-between. Treatment has consisted of soft tissue techniques similar to those used in fibromyalgia, including but not limited to, dry needling, myofacscial release and trigger point massage, kinesiotape, strapping for stability in sporting endeavours, pressure garment use such as SKINS, BSc, 2XU, venous stockings. Specific exercise regimes more atuned to co-ordination and stability than to excessive non-stabilising stretching, muscle energy techniques, mobilisatinos with movement (Mulligans), thoracic ring relocations (especially good with autonomic symtoms), hydrotherapy, herbal supplementaion such as Devils Claw, Cats Claw, Curcumin and Green Tee. Arnica cream for bruising. Encouragment of non-weight bearing endurance activities such as swimming, and cycling to stimuate the red muscle fibres over the ballistic white muscles fibres, since the latter are preferably used in this movement population. Care and even avoidance of end range movement activity. My good friend Abrahao Baptisita, Brazilian Physiotherapist and researcher, recommends the use of muscle stimulation brain retraining for the prevention of shoulder dislocations - subluxations and patella (knee cap) dislocations.
Sacroiliac Joint
The sacroiliac or pelvic joint is not your typical joint. Rather than being made up of two bones and fibrous tissue encapsulating synovial fluid whose primary function is acting a 'pulley' to muscle action, the sacroiliac joint is a ligamentous fibrous non-conforming articulation with varying degrees of movement depending upon gender and collagen fibre type. A young person with JHS tend to be on one end of the SIJ movement spectrum whereas an elderly man would be on the other end.
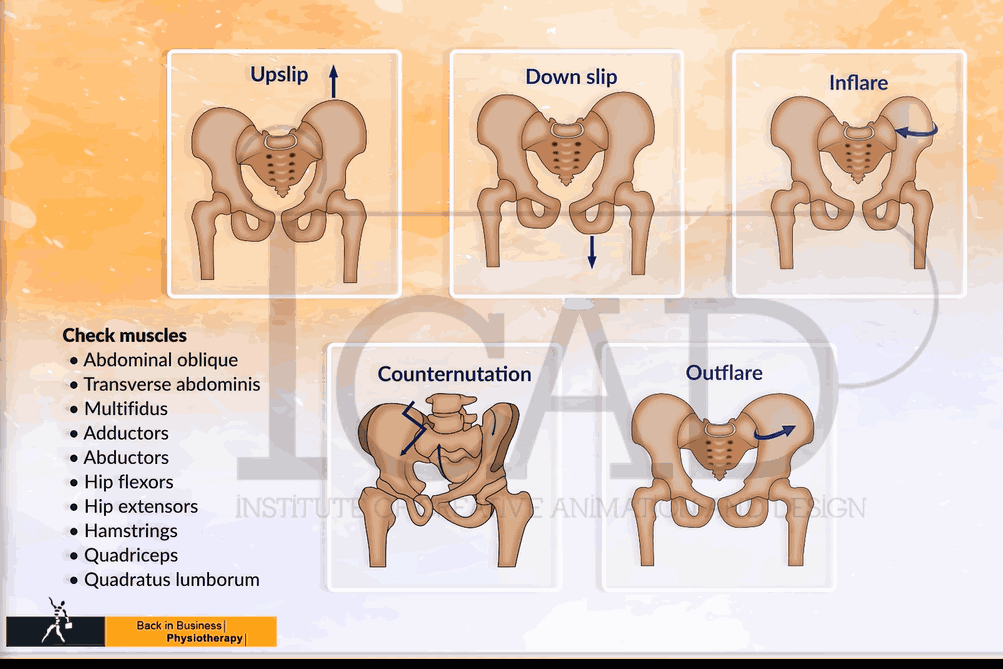
Broad categories of pelvic dysfunction
There are five broad categories of pelvic dysfunction. Some are more common than others. It is important to try to ascertain which dysfunction is present as it will influence treatment and exercise prescription decisions. For example, an 'inflare' may be exacerbated by deep abdominal exercise, an 'outflare' may be exacerbated by hip external rotation exercises, 'downslips' usually don't like traction, and 'upslips' are often confused with 'counternutation'. Both in 'upslips' and 'downslips' the history and mechanism of injury become important.
What constitutes normal and abnormal pelvic alignment? Trauma and muscle imbalance can cause misalignment. Normal walking also may constitute asymmetry which isn't pathological.Actually i find clinically it is better to think of ilia alignment, as the scrum is much smaller,only has one direct muscle attachment and is somewhat hard to conceptual. Although Biochemical purist will probably find the reductionist here simplest and not entirely correct ,the following video hopefully clarify why its easier,clinically,to assess the ilia.
Assessment of the Sacro-iliac Joint should include
- Patrick - FABER test : the patient lies supine on the table, and the examiner stands next to him/her. The examiner brings the ipsilateral hip into flexion, abduction, external rotation so the heel is on the contralateral knee. The examiner fixates the contralateral ASIS and applies pressure on the subjects flexed knee. The test is positive when similar buttock or groin pain below L5 is reproduced (Kokmeyer et al JMPT 2002, 25, 1, 42-8)
- ThighThrust or posterior shear test : the subject lies supine on the table. The examiner flexes the hip and knee so that the hip is at approx 90degrees flexion and slight adduction and the thigh is at right angles to the table with the knee remaining relaxed. One of the examiners hands cups the sacrum and the other arm wraps around the flexed knee. The axial pressure applied is directed through the long axis of the femur, which causes anterior ot posterior shear to the SIJ. The test is positive when familiar pain is provoked over the posterior aspect of the SIJ below L5 (Kokmeyer et al 2002, Laslett et al 2003, 2005)
- Restricted abduction test : the subject is positioned in supine with the leg fully extended and abducted to 30degrees. The examiner holds the ankle and pushes medially while the subject pushes laterally. The test is positve when similar pain is produced over the SIJ below L5 (Broadhurst & Bond, J Spinal Dis, 1998, 11, 4, 341-5). These authors claimed 87% sensitivity and 100% reliability for this test.
- Standing flexion test : is performed by palpating the PSISs whilst the subject is bending forward from the standing position. The test is negative where both PSISs move the same amount and positive where one PSIS moves further cranially than the other which means limited movement of the sacrum on the ilium on the side of the superior PSIS (Potter & Rothstein. Physical Therapy,1985, 65, 11, 1671-5)
- Sitting flexion test : is performed as in standing
- One leg standing : is a very useful test for ascertaining Intra Pelvic Torsion (IPT) where weight shift onto one leg is accompanied by anterior shift of the head of the femur. Frequently, an anterior position of the head can be seen in biped standing when palpating from the side. Palpation for increased adductor tone can also be useful to confirm this hypothesis. Increased adductor tone can also later be palpated in supine before testing ASLR. Furthermore, during the standing lumbopelvic flexion test, palpation for anterior positioning of the head whilst simulataneously palpating for counternutation of the SIJ can be useful in determining which comes first - the IPT or the anterior position of the head of femur. Finally, attempts at improved motor control through horizontal fibres of internal oblique & transverse abdominis activation with lateral weight shifting should result in spontaneous improvements in gluteus medius activation, whilst adductor tone should remain low. Besides LBP and Pelvic Girdle Pain (PGP), this can also be an important consideration in someone presenting with lateral hip pain whereby lack of deep core activation and hence gluteus medius activation results in excessive use of the ITB and Tfl. In terms of motor control it is important to recognise that the muscles which contract prior to the onset of movement should be the stabilizers = muscle of anticipation. If a 'prime mover' muscle initiates the movement then it will become the dominant muscle in that synergy of movement. Hence, if the adductor initiates movement it will result in an anterior draw of the head of femur potentially resulting in anterior hip pain, internal rotation and medial knee pain as well as possibly inducing over pronation and/or porlonged pronation in the foot. Additionally, the adductor may rotate the pelvis ipsilaterally in the horizontal plane, inhibit the glutues medius resulting in reduced lumbo-pelvic rhythm. Whether the adductor is responsible for anterior rotation of the ilium (counter-nutation) (anterior hip pain resulting in muscle spasms of the ilicus) and hence intra-pelvic torsion or is a result of counter-nutation can be assessed clinically by palpation of the SIJ-Ilia and the anterior hip-adductor and determining which occurs first.
- Gillet Test : is performed in 1 leg standing whilst the subject pulls their knee up to their chest. A normal result would be for the PSIS to move inferiorly. If the PSIS remains at the same level or drops only slightly or even moves superiorly this is considered as a positive test
- Prone Knee Flexion test : is performed with the patient prone. While the examiner holds both heels, the patients knees are flexed to 90degrees. The leg lengths are compared by examining the left and right soles of the feet in the prone extended and flexed positions. If one leg appears shorter in extension and lengthens in flexion implies an hypothesised posterior ilial rotation (Potter & Rothstein 1985)
Arab et al (Manual Therapy, 14, 213-221) demonstrated fair to substantial inter and intra-rater reliability for individual tests, moderate to excellent reliability for clusters,and substantial to excellent reliability for composites of the above motion palpation and provocation tests
- Stork test : is performed standing on 1 leg as the subject moves the 90 degree flexed knee into hip flexion and hip extension. The PSISs are palpated w.r.t the sacrum and L4. With the hip moving into flexion, inferior movement of the PSIS and ipsilateral rotation of the L4 is expected. With the hip moving into extension, superior movement of the PSIS and contralateral rotation or no movement of the L4 is expected. Hip hitching can also be tested in this position.
- Active Hip Extension test : involves the client prone and extending their straight leg at the hip. Frequently, clients with LBP and PGP present with reversed gluteal : hamstring timing whereby the hamstrings are dominant. The addition of compression anteriorly or posteriorly can glean information w.r.t force closure. A positve result would be improved timing of contraction of the Gluteus Maximus over the hamstrings. Additionally, a reduction in pain and/or the movement feeling easier 'lighter' to do may also occur. Takasaki et al (Manual Therapy, 2009, 14, 484-489) found that the addition of 50N and 100N anterior compression resulted in the gluteus maximus coming on sooner (263+-99.5ms vs 183.5+-77.9ms vs 91.5+-49.7ms). Improvements with anterior compression may mean the need for transverse abdominus training. Worsening with anterior compression may mean excessive transverse abdominus contraction. Improvements with posterior compression may indicate the need for deep Multifidus (MF) muscle training. Combinations of anterior and posterior compressionon the ilia resulting in improvements may indicate the need for combined deep MF and Transverse Abdominus training. Compression of the thorax and/or elevation/depression, transverse gliding of specific rib rings can also be used. Palpation for tension in the erector spinae muscles of the L/S and T/S as well as using a 'squeezing technique' around the trigger point of tension may also improve Active Hip/Leg Extension suggesting the need to use techniques (such as relaxation through awareness, trigger point dry needling, fascial release, kinesiotaping, etc) to reduce excessive muscle tension
Therefore ideally, gluteal activation occurs prior to or simultaneously with hamstring activation. Where this does not occur, the therapist should consider
- posterior capsule tightness resulting in anterior translation of the head of femur with gluteal activation (hence reflexogenic inhibition)
- anterior rotation of the ilia (counternutation)
- ischioccocygeus spasms and outflare of the ilia
- neuropathy affecting the gluteal nerves
- excessive psoas major activity
- excessive ribcage tightness and hence sympathetic nervous system activity resulting in firing of the hamstrings (these people will say that no matter how much they stretch they still feel that their muscles are tight)
- intra cortical dyskinesia (see Chronic Low Back Pain for more details)
- ALE and Isometric Latissimus Dorsi testing for force closure :
- Prone Figure of 4 Test: involves the client in prone. The knee is bent to 90degrees and the hip is rotated externally, the hip can also be abducted and finally a combination of abduction and external rotation can be made with the knee at 90degrees flexion. These manouvers result in saggital and transverse iliac rotation in 18-35 year olds (Bussey et al, Manual Therapy, 2009, 14, 520-525)
- Gaenslen's Test : useful test for psoas major length and with some adaptation rectus femoris length.
- Supine -> Sitting Test : originally described by DonTigny (1997) it involves assessing leg lengths in supine and in long sitting. The patient is aided to sitting by puling up with their outstretched hands, so as not to involve the abdominal muscles and to avoid pelvic twisting. Outflares and Inflares should remain unaffected by this test. Leg length discrepency should also remain unchanged from either supine or sitting. During an 'upslip' the affected side will appear to be shorter in either position. The reverse will be true fo a 'downslip'. With rotational malalignment the pelvis no longer moves as a unit. With anterior rotation on the right and posterior rotation of the innominate on the left, the pelvis rotates in the transverse plane to the right creating an apparent shorter right leg in sitting. Note that it is the relative shortening which is important. (Shamberger 2002)
Generally there is little evidence to support the use of the Gillet test, standing flexion test, sitting flexion test, or supine-to-sit test to differentiate between subjects with and without static innominate torsion (Pamela K Levangie 1999, PHYS THER Vol. 79, No. 11, November 1999, pp. 1043-1057). However, these tests in my opinion are easy to do and may provide some useful information when examined in the context of the entire clinical picture. Certainly, in some sports such as cycling and rowing the supine -> sit may provide very useful information when exmined in that context.
Assessment of peripheral strength and flexibility is essential before commencing any Swiss Ball exercises or any other training regime. Symmetry in alignment and muscle balance (endurance versus strength) are important aspects for attaining motor control -
remember the analytical physiotherapist should use their 'clinical reasoning' skills to take into account the entire clinical picture
are the muscles short and weak and therefore require strengthening, stretching and power ( i.e. bulk)?
are the muscles long and weak and therefore require endurance for stability ? (remember 'floppies' generally don't like endurance exercise - they prefer ballistic sprinting type of activities)
are there muscles which are over-dominant and therefore require enhanced timing and co-ordination?
for example the static assessment of the influence of the hamstrings, tensor fascia lata and rectus femoris on the pelvic tilt (anterior, posterior and lateral),
in terms of motor control, Bernstein's perspective suggests that the constraints of movement are the 'degrees of freedom' which the central nervous system allows for safe and efficient movement to take place. When considering neuro-linguistic programming (NLP), this tautology of words presents an interesting aspect of communication and goal setting for the physiotherapist. Also don't invoke 'fear' in your clients by using 'instability' without adequate explanations.
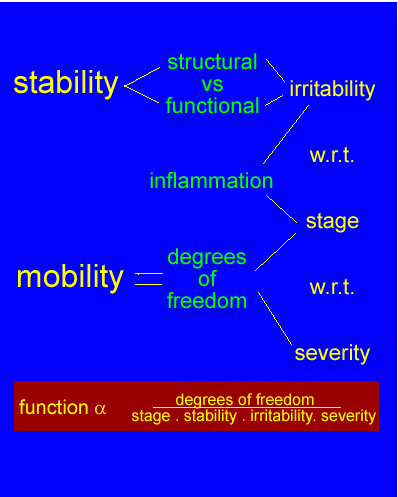
An adapted Geoff Maitland approach to stability and function, incorporating a modified concept of 'degrees of freedom', where the clients reaction to pain determines functional ability.

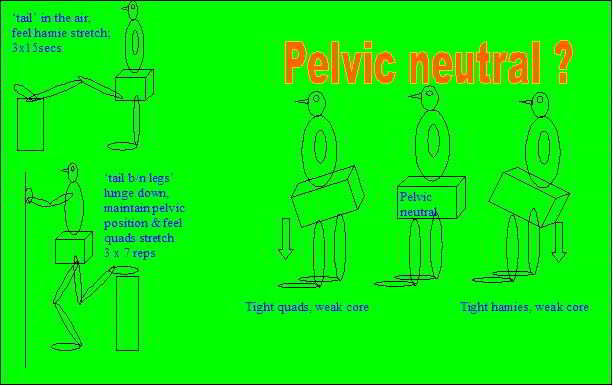
note the excessive scoliosis from the TFL stretch!!!!!
note the excessive posterior pelvic tilt from the hamstring stretch!!!

are the hamies and quads tight because they are weak?
- remember the peroneals, the lateral hamstrings (biceps), the sacrotuberous ligament, erector spinae and deep thoracolumbar fascia are functionally continuous (Dianne Lee 1999)
Following a static assessment, dynamic movement analysis should occur. How does the client walk, run, lift, swim? What is the lumbo-pelvic control and what is the timing between the muscles? For example, do the hamstrings activate before the gluteus maximus? This is frequently the case in hamstring dominant people or people with an anterior iliac rotation whereby counternutation of the SIJ seems to inhibit the gluteus maximus. On the other hand posterior pelvic tilt may be the result of excessive hamstring and rectus abdominis - external oblique activity and a dysfunctional kyphotis low lumbar spine (flexion impairment) whilst anterior pelvic tilt is the result of excessive erector spinae activity (active extension impairment). What is the timing between the erector spinae muscles with arm movements and rocking movements? Can this timing be enhanced by activation of pelvic floor muscles? Is there reduced hip extension (due increased Iliopsoas activity) causing ipsilateral pelvic rotation (in the horizontal plane) resulting in shortening of the contralateral piriformis muscle? This latter scenario may be accompanied with ipsilaterally reduced Prone Knee Bend (PKB) and reduced contralateral Straight Leg Raise (SLR). When extending the hip in prone with a flexed knee does the lumbar spine hyperextend at an unstable segment or rock to one side as can occur with an 'active extension impairment' with it's mal-adaptive spinal stabilising coactivation of erector spinae and iliopsoas?
Any movement discrepancy observed , should be confirmed using special tests such as one leg standing - pelvic control. Additionally, manual muscle testing as well as muscle energy techniques, myofascial dry-needling and joint mobilisations can confirm or negate the 'working hypothesis' of what is causing the dysfunction. The physiotherapist needs to engage the client, thereby educating them to a point where they are able to do their own assessment of the efficacy of any exercise regime or treatment intervention.

reinforcement of shoulder rotation (throwing action) with transverse abdominis activation
- note pelvic tilt and external rotation of stance leg: ?due to tight piriformis and weak gluteus maximus? ?due to hip stiffness? ?due to weak gluteus medius and weak hip rotators?

muscle energy techniques {MET} (gentle [<20%max] and only 3 reps for approx 10 secs)

rectus femoris and iliopsoas


The iliopsoas is frequently regarded as a key player in the compromise of hip extension, lumbar spine lateral flexion, flexion and/or extension. Although clinically, MET's to the iliopsoas can be very useful for restoring lumbar range of movement, there is little evidence to suggest that the iliosoas is tight, too strong or too weak. Similarly, in the abscence of an 'upslip' there is little evidence to suggest it's involvement in anterior pelvic tilt, rather it is more likely to be a posterior pelvic tilter. When separating the two muscles, the iliacus has an anterior rotation affect on the ilium (counternutation), whereas the psoas major has a posterior rotating affect on the ilium. Additionally, the iliacus muscle and posterio-medial aspect of the psoas major are more linkley to have stabilising functions as they are close to the joint and hence axis of rotation, whereas the antero-lateral psoas major may have a largely mobilising-power generating function. If this is the case, then the iliopsoas may be involved with functional synergies which involve the superficial abdominal muscles in maintaining the pelvic neutral position. When a forward/backward rocking motion is performed in standing, the erector spinae and superficial abdominal muscles exhibit reciprocal timing suggesting that the duration of the considerable compressive force generated by the erector spinae can be reduced in the lumbar spine through enhanced superficial abdominal muscle timing. Similarly, reduced erector spinae and enhanced superficial abdominal activity may reduce the amount of compressive forces (excessive force closure) generated on the lumber intervertebral discs. However, more ideally, it is the non-torque producing muscles of the abdominal cavity such as the horizontal fibres of interanl oblique and transverse abdominis as well as the deep fibres of multifidus which maintain lumbar spine neutral posture. By reducing the activation of both superficial abdominals and erector spinae it may be possible for the low threshold muscles to function during postural and endurance activities. During high threshold dynamic exercise such as running, transverse excursion of the diaphragm becomes essential to efficient movement as abdominal expansion may lead to loss of pelvic control. Since the oblique abdominal muscles arise from the lower 6 ribs, the oblique abdominal muscles require adequate length for inferior lateral chest expansion to take place. Notably, the low thoracic spine is covered by the pars thoracic aspect of the erector spinae and hence these muscles require sufficient relaxation for rib excursion to take place. Therefore, it makes sense for the iliopsoas to provide powerful hip/lumbopelvic stability, in a functional synergy with the gluteal muscles during activities such as sprinting and hill running. Despite these paradoxes, it is highly likely that the clinical effect of MET's on the iliopsoas is a proprioceptive one, rebalancing the stabilising synergies of the hip and lumbar spine. Importantly, by including inferior lateral breathing in an iliopsoas release, the therapist will be able to glean the importance of incorrect breathing to the dysfunction. Realistically, the clinical reasoning process allows for such areas of uncertainty by using the correlation between the impairment and disability measures to assess the validity of involving the iliopsoas muscle in the treatment process.
Myofascial dry needling techniques can also be used to reduce muscle tension (spasms) in the superior gluteus maximus, rectus femoris, vastus lateralis/ITB/Tfl, adductor and piriformis muscles.
Additionally, the ilium should be examined for outflares and a tight piriformis, or inflares and a tight iliacus. If both piriformi are contracted then forward flexion may be very difficult. Muscle energy techniques can be used on these muscles. Additionally, adductor longus should be assessed together with the medial hamstrings. Remember, what is tight may also be weak. Therefore, do not increase ROM at the expense of stability. Adductor longus and contralateral external oblique form a functional sling (Diane Lee 1999). Don't forget that the adductor muscles have trigger points which can refer pain into the anus and genital areas (see Travel & Simmons).
Lumbar Spine - Pelvic Kinematics
Sacral nutation & counternutation
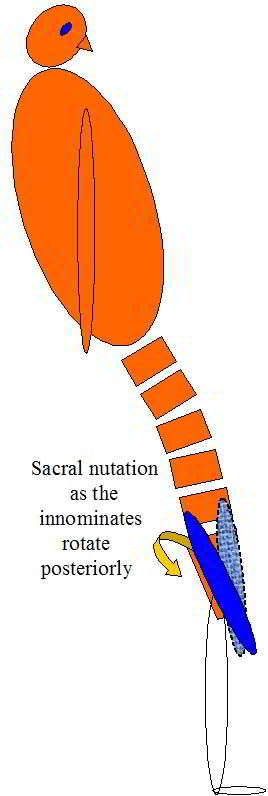
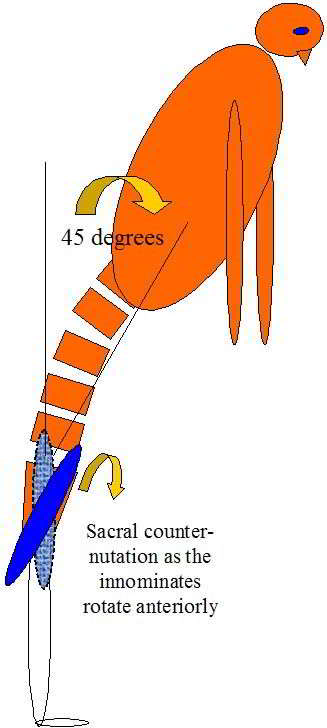
Sacral nutation and counternuation are considered normal events during flexion and extension in standing. It should be noted that counternutation of the sacrum generally occurs beyond 45degrees flexion (some variation between individuals and pathology) and is a movement of the innominates relative to the sacrum. In extension the reverse occurs whereby the ilia rotate posteriorly w.r.t the sacrum resulting in nutation. During extension in sitting, initially the ilia do not rotate whilst the sacrum nutates until all the slack is taken up by the ligaments and pelvic floor muscles at which point the ilia will begin to rotate anteriorly.
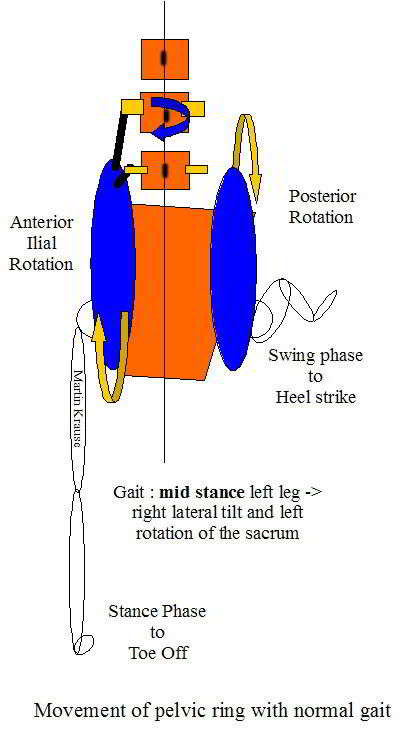
Gait Cycle and Pelvic Rotation
Posterior and lateral view of gait - rotation and counter-rotation of the sacrum/pelvis and spine. As the innominate rotates anteriorly it pushes the sacrum forward on that side so that by toe off the sacrum is rotating in the opposite direction to the pelvis. In the above example, the pelvis rotates to the left as the left leg goes 'swing phase' extension, this pushes the left innominate against the left side of the sacrum, thereby creating right sacral rotation (the exact opposite of pelvic rotation). Lateral tilt is controlled through the medial and lateral slings, whilst the pelvic rotation is controlled by the elements making up the 'spiral sling' (a combination of anterior, posterior and medial-lateral). Inherent in this mechanism are also the hip external rotators, which through the connection of the myofascia and obturator internis, engages the pelvic floor in a stabilising activity.
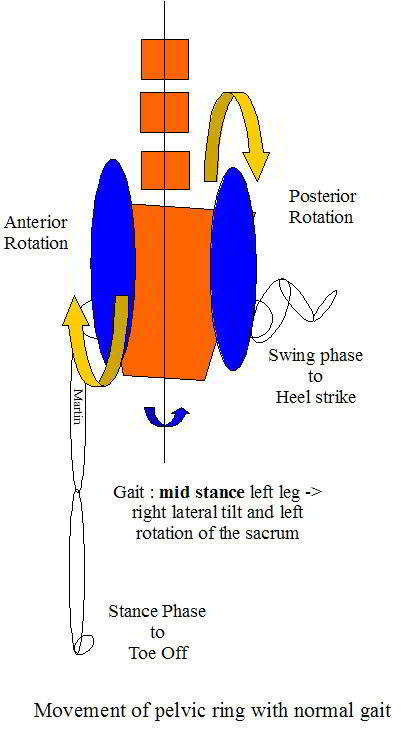
Heel strike is accompanied by a 'locking mechanism' whereby the posterior rotation of the innominate (ilium) is locked with the sacrum through muscular elements on the stance side and the forward push of the opposite innominate (ilium) on the sacrum, on the swing side. Hence as one side goes into 'toe off' 'unlocking' and swing phase, a constant torsion in the sacrum will occur. The amount of sacral torsion will vary depending on ligamentous laxity, muscle balance, terraine and stride length. The Hamstring mechansim across the sacrotuberous and long dorsal ligament contributes to the 'locking' through the 'posterior sling'. During the transition to the unlocking phase anterior 'slings' become important. Mid stance requires control of rotation and pelvic tilt. The inverse dynamics of the kinetic chain of the lower limb mean that every element (Foot -> Pelvis) needs to be considered when assessing pelvic dysfunction.
Posterior view of innominate anterior and posterior rotation, from mid stance to hip extension the sacrum commences to rotate in the opposite direction to the rotation of the pelvis
Anterior innominate rotation with hip extension coincides with ipsilateral pelvic rotation, contralateral spinal lateral flexion and contralateral spinal rotation. Anterior innominate rotation encourages contralateral L4 rotation through attachments of the ilio-lumbar ligaments, which is in turn accompanied by the posterior ilial rotation on the opposite side.These movements occur around an oblique axis. In the above example rotation around the right oblique axis results in a 'counter-rotation' action whereby the right anterior ilial rotation is accompanied by a 'counterlocking' left posterior ilial rotation. As the right hip moves into extension, anterior rotation of the right ilia results in contralateral left sacral torsion (whilst the pelvis is still rotating to the right). The posterior rotation of the left ilia stabilises the left SIJ joint in preparation for heel strike through the tightening of the right sacrotuberous, sacrospinous and interosseous ligaments. The continuation of the biceps femoris mechanism with the sacrotuberous ligament may also act as a mechanical stabiliser. Alternatively, it may be that the sacrotuberous ligament provides powerful proprioceptive input for the biceps femoris. Furthermore, in cases of dysfunction, mechanical hyperalgesia of the sacrotuberous ligament may contribute to reflexogenic muscle spasms in the biceps femoris. This can set up a viscious cycle whereby one perpetuates the other, as shortening and/or incorrect timing of the biceps femoris may result in increased mechanical input (tension) on the sacrotuberal ligament. This can create additional problems elsewhere such as the posterior lateral knee, peroneal nerve, both SIJ's and in the spine.
Confusing? Just remember that the sacrum torsions in the opposite direction to pelvic rotation due to hip extension (and rotation) forces on the ilium
The sacrotuberous ligment also has strong connections with the posterior thoracolumbar fascia, and muscular attachments of gluteus maximus and piriformis. Hereby, the biceps femoris, the GM and the piriformis can increase ligamentous tension.
As the leg moves into extension, counternutation occurs (in this example on the left) resulting in right sacral torsion but with left pelvic rotation in the horizontal plane
L4 rotation can be tested during 'the stork' test through palpation of the spinous process of L4 and sacral sulcus during long striding. Additionally, control over lateral pelvic tilting on the stance leg can also be tested in various positions of flexion and extension whilst palpating the L4 in order to ascertain any mal-rotation suggesting some unstable L4 element. The L5 can almost be considered the 'meat in the sandwich' of sacral torsions (especially backward ones : left on right, right on left), ilial anterior rotations and L4 mal-rotations affect the bood vessels, nerves and articular processes of the L5.
Pelvic Ring Distortion
Frequently, these people present with an apparent or real leg length discrepency and are sometimes confused for an upslip. Examine people in standing from the front and behind. Make sure you are symmetrical to the persons landmarks. Also be certain which is your dominant eye - use the photographers square fingers technique and determine with which eye there is least movement from the centre of the square when both eyes are open compared to one eye shut. Additionally, try to glide the hip anteriorly and posteriorly with more and less weight bearing. The hip will appear to glide further posteriorly on the side of anterior innominate rotation. Generally, the entire pelvis will look like it is rotated.
Outflares and Inflares
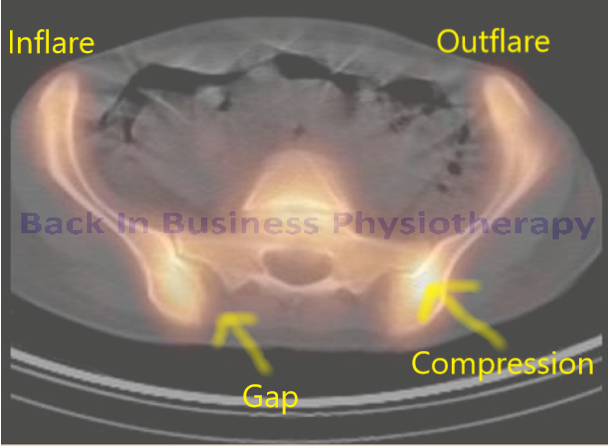
An interesting case of pelvic pain from an outflare right and inflare left of the pelvis causing SIJ compression and gapping respectively. Enhanced bilateral adductor activity, medial right knee pain, gluteal medius weakness and tendinopathy on the right and hamstring insertional tendinoathy on the left were also accompanied by bilateral symphasis pubis inflammation. This 28 year old female suffered from joint hypermobility syndrome. The following are some of the exericses instigated. Additionally the ischiococcygeus was released using pressure relaxation techniques.
Upslips and Downslips
Upslips: can be the result of a sudden vertical force through the outstretched leg for example when stepping into a pot hole, landing awkwardly during a jump or when running. car accidents where the persons foot is on the brake and the force goes up longitudinally through the thigh is also a common mechanism of an upslip. Upslips are generally accompanied by counternutation of the sacrum (anterior rotation of the innominate) which results in tension of the long dorsal sacroiliac ligament. Tightness in the quadratus lumborum and psoas major may contribute to an upslip.
It should be noted that the attachment of the biceps femoris muscle is intimately linked with the continuation of the sacrotuberous ligament and hence can be considered a stabilizer of the SIJ. An MET of the hamstrings are often used to posteriorly rotate the innominates, thereby reducing the counternutation of the sacrum
Downslips: are generally the result of a traction injury such as a rider falling off a horse with the foot caught in the stirrups. I consider these injuries to be exceedingly rare. In theory these are accompanied by sacral nutation (posterior rotation of the innominate) and tension on the sacrotuberal, sacrospinal and interosseous ligaments.
Anterior rotation of the innominate
Anterior rotation of the innominate may the the result of an injury. However, activation of the iliacus which is an important hip stabiliser will also anteriorly rotate the ilium. Therefore, it may be equally important to have the counterbalancing stabilising muscles such as the horizontal fibres of internal oblique and transverse abdominis acting to stabilising the anterior aspect of the SIJ through compression. This would be particularly important if there were also an 'outflare' present. Additionally, the contralateral external oblique may be important during intermittent and high loading. There may also be a role for Psoas Major in the prevention of excessive anterior ilial rotation?
Anterior rotation of the innominate may also occur as a result of adductor muscle tension shifting the head of the femur forward. As the iliacus attempts to stabilise the hip, it counternutates the SIJ resulting in sacral rotation/torsion to the opposite side and pelvic rotation to the ipsilateral side. This can result in compression of the SIJ on the opposite side and hence localised pain there. Therefore, always check OLS (one leg standing) for anterior hip positioning.
Sacral Torsion
Sacral torsion around the oblique axis
The piriformis originates on the anterior aspect of the sacral base and creates a posterior rotation relative to the ilium, whereas the iliacus rotates the ilium anteriorly relative to the sacrum. Either of these movements would create a wedging of the anteriorly wider sacrum against the ilium and would under normal conditions help stabilise the SIJ. However, excessive compression could result in loss of SIJ movement. Inbalance or weakness or inco-ordination in timing, could result in excessive movement.
Palpation in prone : the left sacral sulcus is anterior whereas the right sacral apex is posterior resulting in forward rotation
Shamberger (2002) described these as 'backward rotations' where the base rotates back instead of forwards. Whereas forward rotation accentuates a lumbar lordosis, backward rotations reduce it and may even create a segmental low lumbar kyphosis. In the Osteopathic literature, these presentations have been linked to seemingly unrelated problems such as headaches, disturbed function of the GIT (diarhoea alternating with constipation) and genitourinal problems (frequency, nocturia and a disturbance in menstrual function)
It should be noted that this type of lateral flexion (i.e. on 2 legs and instigated from the spine above) is very different to the type of lateral flexion which occurs during stance phase of walking (inverted pendulum) where the hip rotation dictates the pelvic - spinal mechanics, and where pendular arm swing dictates thoracic movement and hence lumbar mechanics as well.
People with sacral torsions may have increased force closure in one SIJ and reduced forced closure on the contralateral side. Furthermore, they may present with poor form closure on either side (more likely on the side of counternutation) resulting in pain and load transfer dysfunction.
Since pelvic tilt plays an integral role in the oblique torsions during weight bearing it would make sense that the anterior, posterior and medial fibres of the gluteus medius are activated to control the movement of the ilia on the hip.
Bilateral tightness of the piriformis may reduce sacral nutation, whereas asymmetrical piriformis action can axially rotate the sacrum resulting in excessive compression in the contralateral SIJ. Is there piriformis insufficiency due to outflare created by ischiococcygeus? Are they 'buttock clenchers'? Clinically, improving SIJ stability by inhibiting tonically active muscles and activating tonically inhibited muscles (eg multifidus, transverse abdominis) usually improves lateral hip rotator strength.
Check timing between the gluteus maximus and hamstrings (hamies should not be dominant). If the ilium is in anterior rotation it is very difficult for the gluteus maximus to contract.
Can the hip stabilise on lateral weight shift onto a stable ilium? If the ilium goes into anterior rotation (counternutation) then the acetablum may contact the superior-anterior surface of the head of femur resulting in anterior hip pain. Additionally, excessive uncontrolled lateral weight shift places greater strain on the hip lateral stabilisers such as ITB/Tfl possibly resulting in lateral hip pain such as trochanteric bursitis and tendonosis.
Do the opposite femoral nerve (neural dynamics), external rotators (sacral torsion or ilial outflare) and rectus femoris (anterior innominate rotation) create excessive pressure on the opposite SIJ?
If there is an ipsilateral anterior innominate rotation with jamming up of the SIJ concommitant with contralateral hip internal rotation tightness with some adverse neural dynamics of the femoral and sciatic nerves then METs of the hamstrings and external rotators may reposition the innominate and sacrum. In this position the lumbar and thoracic spines can also be palpated. Thoracic rib tightness may be an indication of sympathetic nervous system hypervigilence/dysfunction which may lead increased mechanosensitivity in the muscles innervated by these regions. It is important to do one step at a time before arriving in this position.
Is the sacrum in too little nutation due to lack of multifidus activation? Reflexogenic inhibition and atrophy due to pain or is there excessive muscle spasm?
is there a leg length discrepancy or pubic symphysis instability?
- due to poor hip/pelvic/trunk control?
- due to poor biomechanics of the foot?
-
due to poor knee dynamics?
Osteitis Pubis may present as groin pain. Inflammation of the the bone leads to softening of the bone and cartilage leading to considerable disability. The time frame for recovery is anywhere from 5 months to 2 years. Aetiology is generally from excessive adductor action in activities such as kicking, sitting too high in the saddle of a bike and/or a poor saddle, forced abduction such as skiing, poor inner core stability (transverse abdominis and horizontal fibres of internal oblique) and poor outer sling co-ordination around the pelvis and lumbar spine. However, don't ignore lower limb mechanics such as excessive pronation of one foot and supination of the other. Imbalances between the adductors and the contralateral gluteus medius and the internal and external obliques can play a significant role in poor recovery and may have been part of the aetiology. Inferolateral abdominal wall hernias or weaknesses may have also be the cause of osteitis pubis.
Upslips and Downslips of the ilium are also possible, which maybe accompanied by symphysis pubis shearing (osteitis pubis). Counternutation of the ilium may be accompanied by an upslip or mistaken for an upslip. What is the mechanism of injury? Check quadratus lumborum, external oblique, adductor longus and latissimus dorsi-thoracolumbar fascia for length, strength and 'timing'.
Check stability in Stork test and modified Trendelenburg's test
Palpate conjoint tendon, pubic symphysis and the SIJ
Do the squeeze test at 30, 45 and 60degrees of knee flexion in supine crook lying. Add some rectus abdominus (stomach crunch) to see if it isn't a conjoined rectus abdominus tendonopathy as well.
Do active SLR and check symphysis pubis, then reassess with anterior or posterior ilia compression to ascertain the affect of improved force closure. Reduced pain or easier elevation with anterior compression may be indicative of the need to train the transverse abdominis and horizontal fibres of internal oblique (inner core). Conversely, improvements with posterior compression may be indicative of the need to train the deep multifidus which aids sacral nutation and/or train the muscles and fascia of the posterior outer sling.
- in clients with excessive force closure this can be -ve
- in clients with reduced force closure this can be +ve
- are they getting medial knee pain due to adductor dysfunction?
Do active straight leg raise (ASLR) with or without anterior or posterior compression of the ilia to ascertain 'force closure'. Combinations of anterior and posterior compression on opposite sides is also extremely useful where a sacral torsion is involved. Improvements with anterior compression may mean the need for transverse abdominus training. Worsening with anterior compression may mean excessive transverse abdominus contraction. Improvements with posterior compression may indicate the need for deep Multifidus muscle training. Combinations of anterior and posterior compression resulting in improvements may indicate the need for combined deep MF and Transverse Abdominus training.
The effects of manual pelvic compression on trunk motor control during an active straight leg raise in chronic pelvic girdle pain subjects.
Beales DJ, O'Sullivan PB, Briffa NK. Man Ther. 2010 Apr;15(2):190-9. Epub 2009 Nov 28.
Abstract
A sub-group of pelvic girdle pain (PGP) patients with a positive active straight leg raise (ASLR) responds positively to the application of external pelvic compression during the test. This study investigated the effect of this phenomenon on electromyographic (EMG) activity of the trunk muscles and intra-abdominal and intra-thoracic pressures in subjects with a unilateral sacroiliac joint (SIJ) pain disorder (n=12). All subjects reported reduced difficulty ratings during an ASLR with pelvic compression (paired t-test: p<0.001), yet no statistically significant changes in the muscle activation or pressure variables were found. However, visual inspection of the data revealed two divergent motor control strategies with the addition of compression. Seven subjects displayed characteristics of a decreased EMG profile, while in the other five subjects the EMG profile appeared to increase. As such this study provides preliminary evidence of two disparate patterns of motor control in response to the addition of pelvic compression to an ASLR. The findings may reflect different mechanisms, not only in the response to pelvic compression, but also of the underlying PGP disorder.
Additionally, pressure through the thorax and/or leveation/depression/transverse gliding of specific rib rings can be quite useful to ascertain the influence of rib malalignment and minor instability on ALSR. This again gives immediate diagnostic relevance as well as giving immediate awareness to the client of the existence of a problem.
Compressor Belts for the pelvis may also be useful for some people, however they should only be seen as a means to an end i.e. allow the possibility to function..

The use of pressure through the thorax and ilia can be also be used whilst assessing the clients specific relevant movement problem.
Altered motor control strategies in subjects with sacroiliac joint pain during the active straight-leg-raise test.
O'Sullivan PB, Beales DJ, Beetham JA, Cripps J, Graf F, Lin IB, Tucker B, Avery A., Spine (Phila Pa 1976). 2002 Jan 1;27(1):E1-8.
Abstract
STUDY DESIGN: An experimental study of respiratory function and kinematics of the diaphragm and pelvic floor in subjects with a clinical diagnosis of sacroiliac joint pain and in a comparable pain-free subject group was conducted.
OBJECTIVE: To gain insight into the motor control strategies of subjects with sacroiliac joint pain and the resultant effect on breathing pattern.
SUMMARY OF BACKGROUND DATA: The active straight-leg-raise test has been proposed as a clinical test for the assessment of load transfer through the pelvis. Clinical observations show that patients with sacroiliac joint pain have suboptimal motor control strategies and alterations in respiratory function when performing low-load tasks such as an active straight leg raise.
METHODS: In this study, 13 participants with a clinical diagnosis of sacroiliac joint pain and 13 matched control subjects in the supine resting position were tested with the active straight leg raise and the active straight leg raise with manual compression through the ilia. Respiratory patterns were recorded using spirometry, and minute ventilation was calculated. Diaphragmatic excursion and pelvic floor descent were measured using ultrasonography.
RESULTS: The participants with sacroiliac joint pain exhibited increased minute ventilation, decreased diaphragmatic excursion, and increased pelvic floor descent, as compared with pain-free subjects. Considerable variation was observed in respiratory patterns. Enhancement of pelvis stability via manual compression through the ilia reversed these differences.
CONCLUSIONS: The study findings formally identified altered motor control strategies and alterations of respiratory function in subjects with sacroiliac joint pain. The changes observed appear to represent a compensatory strategy of the neuromuscular system to enhance force closure of the pelvis where stability has been compromised by injury.
Motor control patterns during an active straight leg raise in chronic pelvic girdle pain subjects.
Beales DJ, O'Sullivan PB, Briffa NK. Spine (Phila Pa 1976). 2009 Apr 20;34(9):861-70.
Abstract
STUDY DESIGN: Repeated measures.
OBJECTIVE: To investigate motor control (MC) patterns in chronic pelvic girdle pain (PGP) subjects during an active straight leg raise (ASLR).
SUMMARY OF BACKGROUND DATA: The ASLR is a test used to assess load transference through the pelvis. Altered MC patterns have been reported in subjects with chronic PGP during this test. These patterns may impede efficient load transfer, while having the potential to impinge on respiratory function and/or to adversely affect the control of continence.
METHODS: Twelve female subjects with chronic PGP were examined. Electromyography of the anterior abdominal wall, right chest wall and the scalene, intraabdominal pressure, intrathoracic pressure, respiratory rate, pelvic floor kinematics, and downward leg pressure of the nonlifted leg were compared between an ASLR lifting the leg on the affected side of the body versus the nonaffected side.
RESULTS: Performing an ASLR lifting the leg on the affected side of the body resulted in a predominant MC pattern of bracing through the abdominal wall and the chest wall. This was associated with increased baseline shift in intraabdominal pressure and depression of the pelvic floor when compared with an ASLR lifting the leg on the nonaffected side.
CONCLUSION: This MC pattern, identified during an ASLR on the affected side of the body, has the potential to be a primary mechanism driving ongoing pain and disability in chronic PGP subjects.
The effect of increased physical load during an active straight leg raise in pain free subjects.
Beales DJ, O'Sullivan PB, Briffa NK. J Electromyogr Kinesiol. 2010 Aug;20(4):710-8. Epub 2010 Jan 20.
Abstract
PURPOSE: It has been proposed that pelvic girdle pain (PGP) subjects adopt a high load motor control strategy during the low load task of the active straight leg raise (ASLR). This study investigated this premise by observing the motor control patterns adopted by pain free subjects during a loaded ASLR (ASLR+PL).
METHOD: Trunk muscle activation, intra-abdominal pressure, intra-thoracic pressure, pelvic floor motion, downward pressure of the non-lifted leg and respiratory rate were compared between resting supine, ASLR and ASLR+PL. Additionally, side-to-side comparisons were performed for ASLR+PL.
RESULTS: Incremental increases in muscle activation were observed from resting supine to ASLR to ASLR+PL. During the ASLR+PL there was a simultaneous increase in intra-abdominal pressure with a decrease in intra-thoracic pressure, while respiratory fluctuation of these variables were maintained. The ASLR+PL also resulted in increased pelvic floor descent and greater downward pressure of the non-lifted leg. Trunk muscle activation was comparable between sides during ASLR+PL in all muscles except lower obliquus internus abdominis, which was more active on the leg lift side.
CONCLUSION: Pain free subjects respond to an ASLR+PL by a general increase in anterior trunk muscle activation, but preserve the pattern of greater activation on the side of the leg lift observed during an unloaded ASLR. This contrasts to findings in PGP subjects who, despite having a high load strategy for performing an ASLR on the symptomatic side of the body, display equal bilateral activation of the anterior abdominal wall during the ASLR. This differentiates PGP subjects from pain free subjects, supporting the notion that PGP subjects have aberrant motor control patterns during an ASLR.
Changes in pelvic floor and diaphragm kinematics and respiratory patterns in subjects with sacroiliac joint pain following a motor learning intervention: a case series.
O'Sullivan PB, Beales DJ. Man Ther. 2007 Aug;12(3):209-18. Epub 2006 Aug 17.
Abstract
This study was a case series design. The objectives of the study were to investigate the ability of a motor learning intervention to change aberrant pelvic floor and diaphragm kinematics and respiratory patterns observed in subjects with sacroiliac joint pain (SIJP) during the active straight leg raise (ASLR) test. The ASLR test is a valid and reliable tool to assist in the assessment of load transference through the pelvis. Irregular respiratory patterns, decreased diaphragmatic excursion and descent of the pelvic floor have been reported in subjects with SIJP during this test. To date the ability to alter these patterns has not been determined. Respiratory patterns, kinematics of the diaphragm and pelvic floor during the ASLR test and the ability to consciously elevate the pelvic floor in conjunction with changes in pain and disability levels were assessed in nine subjects with a clinical diagnosis of SIJP. Each subject then undertook an individualized motor learning intervention. The initial variables were then reassessed. Results showed that abnormal kinematics of the diaphragm and pelvic floor during the ASLR improved following intervention. Respiratory patterns were also influenced in a positive manner. An inability to consciously elevate the pelvic floor pre-treatment was reversed. These changes were associated with improvement in pain and disability scores. This study provides preliminary evidence that aberrant motor control strategies in subjects with SIJP during the ASLR can be enhanced with a motor learning intervention. Positive changes in motor control were associated with improvements in pain and disability. Randomized controlled research is required to validate these results.
The aim is the correction of pelvic mal-alignment & asymmetry - both static and dynamic


note the very poor trunk posture on hamstring stretching and the anterior pelvic tilting on quads stretching!!! - he will never make the hurdling team
What is the influence of the global stabilisers? In particular, external oblique and latissimus dorsi. As well as external oblique and adductor longus. Remember that the gluteal maximus works synergistically with the contralateral latissimus dorsi/erector spinae/thoracolumbar fascia during gait.
Altered breathing patterns during lumbopelvic motor control tests in chronic low back pain: a case–control study
Nathalie Roussel, Jo Nijs, Steven Truijen, Liesbet Vervecken, Sarah Mottram, and Gaëtane Stassijns
Abstract
The objective of the study was to evaluate the breathing pattern in patients with chronic non-specific low back pain (LBP) and in healthy subjects, both at rest and during motor control tests. Ten healthy subjects and ten patients with chronic LBP participated at this case–control study. The breathing pattern was evaluated at rest (standing and supine position during both relaxed breathing and deep breathing) and while performing clinical motor control tests, i.e. bent knee fall out and active straight leg raise. A blinded observer analyzed the breathing pattern of the participants using visual inspection and manual palpation. Costo-diaphragmatic breathing was considered as optimal breathing pattern. Subjects filled in visual analog scales for the assessment of pain intensity during the tests. At rest, no significant differences were found between the breathing pattern of patients and healthy subjects (P > 0.05). In contrast, significantly more altered breathing patterns were observed in chronic LBP-patients during motor control tests (P = 0.01). Changes in breathing pattern during motor control tests were not related to pain severity (P > 0.01), but were related to motor control dysfunction (P = 0.01).
Is the thoracic spine mobile enough to allow localised movements without placing excessive movement on the lumbar spine? Additionally, lack of lateral chest expansion will affect the role of the diaphragm in respiration and stabilisation. Suggestions have been made that people who hyperventilate create respiratory alkalosis which results in metabolic acidosis and therefore creates excessive tension in the soft tissue through the sympathetic innervation of the blood vessels. Finally, lack of low thoracic spine mobility may affect the nutrition to the nerves innervating the muscles and blood vessels of the abdominal and pelvic region. Therefore, it is imperative to assess the mobility of the thoracic spine. Additionally, check the patency of the femoral artery in the groin region. A discrepancy in pulse rate and pressure may suggest that the iliopsoas is restricting blood flow. An MET of the iliopsoas can confirm or negate this hypothesis. Adhesion formations may be another reason. Moreover, reduced lateral diaphragmatic movements and reduced inferior thoracic spine mobility may be affecting sympathetic nervous system blood vessel tone and hence the patency of the pulse. It could be envisaged that reduced blood flow would affect the deep endurance stabilising muscles of the leg.
These exercises are designed for people with an anterior pelvic tilt or Posterior Pelvis (PPXS). They should be proceeded by low threshold diaphragmatic and pelvic floor exercises which enhance low loading IAP (intra abdominal pressure). Generally, people with PPXS are 'floppy' or of low muscle tone and need to be 'energised'.
What happens to the vertebrae and paraspinal muscles when lifting the leg or arm or both? There should NOT be an increase in erector spinae tension in the thoracolumbar regions nor should there be an inhibition of diaphragmatic movement.
People with APXS tend to be of high muscle tone. It is important to assess their anterior abdominal wall for excessive tightness and reduce this for optimal diaphragmatic expansion.
Both in APXS and PPXS the thoracic biomechanics and myo-mechanics needs to be assesed and treated.
What about 'the needle' exercise from yoga which may be used to assess thoracic spine rotation
These high threshold loading exercises should only be done when control over the diaphragm and pelvic floor is achieved in low threshold scenarios. They do not replace those abilities. Low threshold function needs to be continually emhasised even after achieving a stage where high threshold loading exercises are required. The second exercise above should be done in sitting either in a chair or on a Swiss Ball. If using a Swiss Ball the person can move it gently from side to side whilst maintaning the isometric contraction. The third exercise above should only be undertaken once lateral weight shifting and OLS (one leg standing) control are optimal. The aim is to combine the internal corset stability (tr abdo, hori fibres int oblique, diaphragm and pelvic floor) with the external slings. The Gluteus Medius should function optimally over and above ITB - TFL strain and tension. In fact assessing the internal corset 'guy wires' and their ability to improve sings synergies can be tested in side lying and using 'the clam' exercise', in supine using ASLR and in prone using ALE
Connell AT (2008) Concepts for assessment and treatment of anterior knee pain related to altered spinal and pelvic biomechnics: a case report. Manual Therapy, 13, 560-563. This author used 3 sessions of treatment to the T10/11, T11/12, T12/L1 and L5/S1 to improve the ROM and ability to squat in a patient with anterior knee pain.
Grindstaff TL et al (2009) Effects of lumbopelvic joint manipulation on quadriceps activation and strength in healthy individuals. Manual Therapy, 14, 415-420. These investigators found a significant increase in the ability to produce quadriceps force (+3%) and activation (+5%) immediatley following lumbopelvic joint manipulation
When dealing with diaphragm dysfunction which is located in the regions T7-L3 and thoracolumbar dysfunction the innervation of these regions should be considered. Don't forget that the diaphragm is innervated by C3,4,5 whilst the latissimus dorsi is innervated by the low cervical spine, let alone the inferior trapezius which has an upper cervical spine innervation. Hence don't forget to asssess the cervical spine. Also occulomotor and postural reflexes may be important.
Summary of integrated Pelvis - Body dysfunction
The pelvic floor can be considered as the base of the cylinder which incorporates the pelvis, abdominal muscles, back muscles, the thoracolumbar fascia and diaphragm. Frequently, people presenting with low back and pelvic pain also describe weakness of the bladder. Such weakness may involve the urethra and effective force closure around the pelvis. When a person coughs, the urethra usually contracts with the abdominal muscles thereby avoiding embarrassment. However, stess urinary incontinence occurs in 8.5 - 38% of women (Ashton-Miller et al 2001, Scan J Urology & Nephrology Supp 207). It affects 28% of elite female athletes (Bo & Borgen 2001, Med Sc Sp Ex, 33, 11, 1797), one out of ten males and 4 of every 10 females (Fantl et al 1996, Managing acute and chronic urinary incontinence, clinical practice guidlelines, no2, Rockville MD, US Dep't Health & Human Services). Cyclists can also have pelvic floor dysfunction and neuropathies as a result of direct presure on the pudendal nerves with an incorrect saddle or saddle position. Urinary continence relies on the support of the sphincter closure system and the urethral support system. Essentially, the urethra sits inside a hammock of muscular and fascial and liagmentous support.
The over contraction of the pubococcygeus could result in sacral counternutation. It is likely that the muscles are balanced in such a fashion that optimisation of function occurs - 'not too much and not too little'
We routinely use transabdominal Real Time Ultrasound as an assessment and biofeedback tool for training the synergistic role of the pelvic floor and transverse abdominis muscles. In particular during Active SLR we examine whether there is pelvic floor descent and whether this changes with manual pelvic compression and whether these people can be trained to maintain or raise the pelvic floor during this manouvre. Importantly, lumbar posture and spine neutral may have a significant influence on results. Progression from supine to side lying and to standing with weight shifting are also carried out using R-T US. Coccygodynia can be the result of excessive pubococcygeus activity.
Lee D, Lee L-J (2004) Stress Urinary Incontinence - a consequence of failed load transfer through the pelvis? 5th World Interdisciplinary Congress on Low Back and Pelvic Pain, Melbourne, November 2004
Smith et al (2006) Disorders of breathing and continence have a stronger association with back pain than obesity and physical activity. AJP, 52, 11-16
Sapsford RR et al (2000) Co-activation of the abdominal and pelvic floor muscles during voluntary exercises. Neurourology and Urodynamics, 20, 1, 31-42
Kelly M et al (2007) Healthy adults can more easily elevate the pelvic floor in standing than in crook-lying: an experimental study. AJP, 53, 187-191
Rahmani N & Mohseni-Bandpei MA (2009). Application of perineometer in the assessment of pelvic floor muscle strength and endurance: a reliability study. Journal of Bodywork and Movement Therapies.
Stuge B et al (2006) To treat or not to treat postpartum pelvic girdle pain with stabilizing exercises? Manual Therapy, 11, 337-344.
Hip - retroversion of the acetabulum
Reynolds, Lucas, Klaue (1999). Retroversion of the acetabulum - a cause of hip pain. JBJS, 81B, 2, 281-8
Retroversion of the acetabulum can lead to increased ROM of internal rotation with a conommittant loss of external rotation which in turn affects pelvic rotation during activitis such as ambulation.
Cam and Pincer Lesions can occur in association with labral lesions. Excessive tension in the external hip rotators can cause anterior acetabular impingement. Iliopsoas tendonosis may be associated with anterior labral lesions. Excessive anterior rotation of the innominate can cause anterior hip impingement.
Pfirrmann et al (Radiology, 240, 3, 2006 pp778-785) used MRI measurements of alpha angles and the depth of the acetabulum to determine the risk and incidence of CAM and Pincer lesions in the hip. They concluded that a deep acetabulum and posteroinferior acetabular cartilage lesions were a characteristic finding of pincer impingement.
Lateral hip pain should always be assessed in terms of internal corset versus external corset stability as outlined by Vleemings muscular 'slings' or neuromuscular vectors.
Muscle energy techniques (adaptation of PNF contract relax)
Muscle energy techniques as developed by British - Canadian physiotherapist, the late David Lamb, used the priciples of contract relax technqiues from PNF to restore pelvic-hip-lumbar spine functional symmetry. The contract relax technique uses the principle of autogenic muscle relaxation post isometric contraction. Theoretically, this is based on Ib tendonous, golgi tendon organ, autogenic inhibition or gate control theory, involving type III muscle afferents. In the PNF concept, this isometric contraction can be up to 100% max, whereas when using MET's the contraction level is usual low and may represent only 10%max when using it to make pelvic and back adjustments. Investigations, comparing static stretching, isometric contractions and contract-relax have demonstrated "a broader adaptive response that likely explains its (C-R) superior efficacy in acutely increasing ROM" (Kay et al 2015, Med Sc Sp Ex, 47, 10, 2181-2190). Clinically, hip flexor C-R are used to improve the ROM of both flexion and extension when used in the Gaelsens position (see previous). When used in side-lying an isometric contraction of the hip flexor which is on the lower side can be used to improve contralateral (upper side) rotation as well as reduce SIJ counternutation. The same position and contraction can be used whilst placing the fingers on the upper side Psoas Major (in the anterolateral abdominal cavity) whilst asking the client to use lateral diaphragmatic breathing to release the myofascia which envelops the hip flexor and diaphragm. Met's can also be performed on the piriformis whilst in Prone Knee Bend to reduce sacral torsion and ilial outflares. Ischiococcygeus releases use a similar principle of isometric contraction with finger pressure, whilst applying a medial pressure to the ASIS to reduce outflares. Whereas, the previous examples involve muscle contractions to improve the ROM in the direction opposite to the muscles normal functional pull, the hamstring is used to improve ilial counter-nutation in the same direction as it's pull. This technique is done in side-lying, where a pressure is applied by the therapist to the lower part of the clients posterior thigh, whilst the client pushes their leg into the therapists hand, the therapists other hand is applying a pressure on the sacral tuberosity in a manner which opposes counter-nutation. Having performed these techniques since the late 1980's I can attest to their clinical efficacy, especially when they are combined with manual therapy joint mobilisations, myofascial releases, dry needling and an appropriate exercise regime.
Trigger Points and Fascia
Recent publications into trigger point therapy include
- Biochemicals associated with pain and inflammation are elevated in sites near to and remote from active myofascial trigger points. Shah JP et al (2008) Arch Phys Med Rehabil, 89, 16 -23.
- Integrated Dry Needling with new concepts of myofascial pain, muscle physiology and sensitization. Shah JP In : Contemporary Pain Medicine, Integrative Pain Medicine, The Science and Practice of Complementary nd Alternative Medicine in Pain Management. Ed Audette & Bailey, Human Press, Totowa, NJ
- An explanation of Simons' integrated hypothesis of trigger point formation. Gerwin RD, Doomerholt J, Shah JP (2004). Current Pain and Headache reports, 8, 468-475
- Uncovering the biochemical milieu of myofascial trigger points using in vivo microdialysis: an application of muscle pain concepts to myofascial pain syndrome. Shah JA & Gilliams EA (2008). J of Bodywork and Movement Therapies, 12, 371-384
- An in-vivo microanalytial technique for measuring the local biochemical milieu of human skeletal muscle. Shah JP et al (2005) J Appl Physiol, 99, 1977-1984
Comparison of normal, latent and active trigger point physiology using microdialysis in the upper trapezius muscle (Shah et al 2005). These researchers also found similar results for Bradykinin, Calcitonin Gene Related Peptide (CGRP), Substance P, Tumor Necrosis Factor alpha, and Interleukin 1beta. Additionally, reduced pH levels were also seen in areas of active trigger points.
However, a number of sites in the myofibrillar complex such as reduce binding sensitivity and capacity of Troponin C for calcium, altered troponin-tropomysosin interaction to impaired binding and force generation by actin and myosin have been implicated in impaired force generation (Green 1990). Indeed, in the absence of any association between relaxation rates and Calcium kinetics raises support for the notion of a rate-limiting process controlling the relaxation of fatigued muscles being located in the contractile proteins (Hill et al 2001). During fatigue the relaxation times can be prolonged as much as 50% (Bigland-Ritchie et al 1986) thus resulting in increased force generation during submaximal stimulation due to tetanic fusion despite a substantial fall in the maximum tetanic force (Bigland-Ritchie et al 1986).
The initial overall loss of force production seen may be due to Desmin and Titan damage (Lieber & Friden 2002). Desmin acts as an extra-sarcomeric mechanical stabilizer between adjacent Z discs and the attachment to the costomere at the sarcolemma (Lieber, Shah & Fridén 2002). The costomere complex contains Talin, Vinculin & Dystrophin which attach to the trans-sarcolemmal proteins Integrin and Dystrophin associated proteins. These proteins allow the lateral transmission of force from actin to the basal lamina containing type IV collagen which is contiguous with the endomysium (Kovanen 2002). Desmin loss after eccentric exercise can occur within 5 minutes, possibly as a result of increased intracellular Calcium leading to Calpain activation and selective hydrolysis of intermediate filament network (Lieber & Fridén 2002). This may result in the ‘popping of sarcomeres' of different length thereby potentially loosing their myofilament overlap of actin and myosin (Lieber & Fridén 2002). Hence, reduced force production would be expected. Additionally, the release of matrix metalloproteinase (MMP) which may degrade the extramyocellular type IV collagen (Korskinen, Kovanen, Komulainen et al 1996). However, this effect occurs many days after exercise (Korskinen et al 1996) and could even effect torque production 28 days after exercise (Lieber & Fridén 2002). This has significant implications in exercise training prescription.
flash file created by Martin Krause 2003
Titan molecules span the gap between the ends of the thick filaments and Z-bands. At the 2007 MPA conference in Cairns, Rob Herbert, provided the AJP oration whereby he explained the significance of Titan as a major determinant of extensibility in muscle fibres. Additionally, he stated that Titan is differentially expressed in human skeletal muscle as short stiff fibres and long compliant fibres
-
Costomeres are 15 different proteins
- Low oxidative muscles have a tendency to tear during eccentric exercise
- Loss of desmin proceeds loss of fibronectin membrane
- Fibre strain results in increased intracellular and extracellular calcium which ?may lead to desmin hydrolysis through calpaine?
- Sarcomere shortening occurs to the detriment of tendon lengthening
- Excitation-contractile coupling may be the area disrupted rather than pure sarcomere disruption
- Structural changes of the disruption of the cytoskeleton include dystrophin (sublaminal membrane protein), sometimes desmin and titin, whereas alpha actin is always OK ?suggesting that calpaine is not the enzyme responsible for protein dysruption?
- Creatine Kinase has no correlation with these cytoskeletal changes
- Inflammatory process important for tissue cleaning and remodelling
- Mechanism for muscle adaptation may be myosin gene regulation - heavy chain myosin isoform upregulation
- Oxygen into the Mitochondria and through the electron transfer chain (ETC) results in ATP use of 20% for power and 80% for heat, therefore people producing less heat may be producing more power?
- Slow twitch muscle fibre concentration varies with the years of training
- Cycling cadence velocity at peak efficiency for slow twitch muscle fibres is 80rpm
Trigger Point palpation
Trigger point - gluteus medius
Trigger Points : piriformis, gluteus maximus, quadratus lumborum, levator ani
Trigger Point - adductor magnus. Note the anal referral which is common amongst cyclists who use the adductors to power hip extension
Trigger Points : Obtrator Internus and pelvic floor
Trigger point - iliopsoas
Fibroblasts and Loose Connective Tissue
At the APA conference in Sydney during October 2009, Dr Helene Longevin presented her research into the effects of stretching subcutaneous tissue. Superficial and deep fascia are composed of loose and dense connective tissue layers. The loose layers allow dense layers to glide past one another. This tissue contains abundant fibroblasts, immune cells and neurovascular bundles. A 20% static stretch of loose connective tissue for 30minutes significantly increases the size of fibroblasts in vivo and in vitro. Although this mechanism remains unclear it is hypothesised to be due to microtubule reorganisation (Beta-tubulin). Inhibition of growth kinase and Roc prevents the cells from spreading out. Actine polymerisation occurs at the leading edge. Fibro-attraction occurs whereby fibroblasts push forward at it's front edge, whilst retracting the rear (through Rho). Both Rac and Rho are activated simultaneously. The fibroblasts microtubule assembly contributes to connective tissue (C.T) relaxation, which means that tense in connective tissue is actively regulated. Viscoelastic response of loose connective tissue is influenced by specific cytoskeletal inhibitors. Rac increases the equilibrium force. Active C.T tensioin regulation may occur normally in response to sustained chnages in tissue length (e.g. hift in body position). This role may be to prevent sustained mechanical stimulation of other cells within the C.T (immune cells, nerve fibres, blood vessels).
The dense C.T fibroblasts don't respond to stretch due to the stiff matrix preventing the fibroblasts from receiving any strain. Scarring due to injury causes an increase in dense C.T which can be pevented by 10minutes, 2 times per day for 1 week in a suspended tail animal model. The combination of reduced movement and inflammation is a recipe for fibrosis. R-T US can be used as feedback during dry needling to observe C.T movement. In people suffering low back pain the fascial layers are less fluid and less differentiated. Additionally, people with LBP have hicker perivascular C.T. Involuntary muscle spasms may decrease the relative C.T motion during passive movement. Conversely, increased C.T thickness, stiffness and/or viscosity may affect the passive stiffness and range of movement of adjacent muscles.
Intrinsic tension within C.T will have profound effects in the cells within it such as blood vessel precursors stimulating angiogenesis. Similarly, immune cells may be affected by this tension. High amplitude or repetitive tissue stretch may cause injury but can also increase C.T strength. Low amplitude stretch within or slightly beyond the usual ROM may help maintain appropriate mibility and dynamic tissue response. Hence this may represent strong eveidence for STM, dry needling, joint mobilisations, muscle energy technqiues, strain-counterstrain techniques and training with Whole Body Vibration.
Bed rest can have deleterious effects on muscle function. Researchers have recently described a direct muscle afferent-pituitary axis whereby bio-assayable growth hormone (BGH) regulation is tightly coupled with muscle function rather than muscle fibre type. Unlike, exercise-induced increases in plasma immuno-assayable growth hormone (IGH), whose concentration peak occurs during or after longer duration aerobic or resistance exercise involving larger muscle mass, BGH is released after a brief series of isometric contraction (McCall et al 2001). The BGH response is absent , despite the maintenance of normal torque output and pre-exercise plasma BGH and IGH, when leg musculature is chronically unloaded, as after 2 days bed rest or space flight. They hypothesised that this was due to chronic alterations in proprioceptive inputs (McCall et al 2001). These responses normalised within approximately 8 days of ambulatory recovery. Furthermore, they suggested that BGH stimulates bone growth and that low threshold fibre activation through electrical stimulation, exercise and /or vibration may ameliorate the effects of chronic unloading (McCall et al 2001). Moreover, this is direct evidence for the existence of a muscle-pituitary functional pathway in the absence of inflammation. It also highlights the need not to underestimate the effects of bed rest when recommencing a training regime after a period of illness or trauma. Furthermore, it would appear that low threshold isometric contractions, as occur during the application of muscle energy techniques, may stimulate this growth hormone.
Good exercise prescription (of power and endurance) considers whether the person is functionally unstable due to weakness, stiffness, atrophy or hypermobility
Check out the 'tensegrity model' as it applies to biomechanical integrety
Clinical example of sacroiliac pain
Further Reading
Bermark (1989) Stability of the lumbar spine: a study in mechanical engineering. Acta Orthopaedica Scandinavica, 230, 60, 20-24
Boyling & Jull (2004) Grieves Modern Manual Therapy, The Vertebral Column, Churchill Livingston
Chaitow L (2001) Muscle Energy Techniques. Edinburgh
Chiarelli PE (1998) Womens waterworks ; curing incontinence. Gore & Osment Publications Rushcutters Bay
Cholewicki & Silfies (2004) Clinical biomechanics of the lumbar spine. In : Boyling & Jull (2004) Grieves Modern Manual Therapy, The Vertebral Column, Churchill Livingston, ch7
Christensen et al (2004) Clinical reasoning in the diagnosis and management of spinal pain. In : Boyling & Jull (2004) Grieves Modern Manual Therapy, The Vertebral Column, Churchill Livingston, ch27
Elvey & O'Sullivan (2004) A contemporary approach to manual therapy. In Boyling & Jull (2004) Grieves Modern Manual Therapy, The Vertebral Column, Churchill Livingston. Ch33
Gibbons & Tehen (2000) Manipulation of the spine, thorax and pelvis. An osteopathic perspective. Churchill Livingstone, Edinburgh
Hides et al (1994) Evidence of lumbar multifidus muscle wasting ipsilateral to symptoms in patients with acute/subacute low back pain. Spine, 19, 2, 165-177
Hides et al (1995) Multifidus recovery is not automatic following resolution of acute first episode low back pain. Spine, 21, 23, 2763-2769
Hodges (1997) Feedforward contraction of transversus abdominis is not influenced by the direction of arm movement. Exp Brain Research, 114, 362-370
Hodges & Richardson (1997) Contraction of the abdominal muscles associated with movement of the lower limb. Physical Therapy, 77, 132-144
Hodges & Gandevia (2000) Changes in intra-abdominal pressure during postural and respiratory activation of the human diaphragm. J Appl Physiol, 89, 967-976
Hodges et al (2002) Feedforward activity of the pelvic floor muscles precede rapid upper limb movements. Australian Physiotherapy Association conference, Sydney, abstract 21
Holstege et al (1996) The emotional motor system. Elsevier, Amsterdam
Kelly M et al (2007) Healthy adults can more easily elevate the pelvic floor in standing than in crook-lying: an experimental study. AJP, 53, 187-191
Lee D, Lee L-J (2004) Stress Urinary Incontinence - a consequence of failed load transfer through the pelvis? 5th World Interdisciplinary Congress on Low Back and Pelvic Pain, Melbourne, November 2004
Lee D (2004) The Pelvic Girdle: an approach to the examination and treatment of the lumbopelvic-hip region. Churchill Livingstone, Edinburgh
Mercer (2004) Kinematics of the spine In : Boyling & Jull (2004) Grieves Modern Manual Therapy, The Vertebral Column, Churchill Livingston, ch4
O'Sullivan (2004) 'Clinical instability' of the lumbar spine: its pathological basis, diagnosis and conservative management. In : Boyling & Jull (2004) Grieves Modern Manual Therapy, The Vertebral Column, Churchill Livingston Ch 22
O'Sullivan et al (2002) Altered motor control in subjects with sacro-iliac joint pain during active straight leg raise test. Spine 27, 1, E1-E8
O'Sullivan et al (2002) The effect of different standing and sitting postures on trunk muscle activity in a pain free population. Spine, 27, 1238-1244
O'Sullivan et al (2003) Lumbar repositioning deficit in a specific low back pain population. Spine, 28, 10, 1074-1079
Panjabi (1992) The stabilizing system of the spine. 1: Function, dysfunction, adaptation, and enhancement. J of Spinal Disorders, 5, 4, 383-389
Potter & Rothstein. Physical Therapy,1985, 65, 11, 1671-5
Rahmani N & Mohseni-Bandpei MA (2009). Application of perineometer in the assessment of pelvic floor muscle strength and endurance: a reliability study. Journal of Bodywork and Movement Therapies.
Richardson et al (2002) The relationship between the transversely oriented abdominal muscles, sacroiliac joint mechanics, and low back pain. Spine, 27, 4, 399-405
Sapsford (2001) The pelvic floor: a clinical model for function and rehabilitation. Physiotherapy, 87, 620-630
Sapsford et al (2001) Co-activation of the abdominal and pelvic floor during voluntary exercises. Neurology and Urodynamics, 20, 31-42
Sapsford & Hodges (2001) Contraction of the pelvic floor muscles during abdominal manouvers. Archives of Physical Medicine and Rehabilitation, 82, 1081-1088
Sapsford & Kelley (2004) Pelvic Floor Dysfunction in low back and sacroiliac dysfunction. In: Boyling & Jull (2004) Grieves Modern Manual Therapy, The Vertebral Column, Churchill Livingston, ch35
Schamberger W (2002) The malalignment syndrome ; implication for medicine and sport. Churchill Livingstone, Edinburgh
Shumway-Cook & Woollacott (1995) Motor control: theory and practical applications. Williams and Wilkins, Baltimore
Smith et al (2006) Disorders of breathing and continence have a stronger association with back pain than obesity and physical activity. AJP, 52, 11-16
Snijders et al (1993) Transfer of lumbosacral load to iliac bones and legs. 1. Biomechanics of self bracing of the sacroiliac joints and its significance for treatment and exercise. Clinical Biomechnics, 8, 285-294
Snijders et al (1993) Transfer of lumbosacral load to iliac bones and legs. 2. Loading of the sacroiliac joints when lifting in a stooped posture. Clinical Biomechanics, 8, 295-301
Stuge B et al (2006) To treat or not to treat postpartum pelvic girdle pain with stabilizing exercises? Manual Therapy, 11, 337-344.
Sturesson et al (2000). A radiostereometric analysis of movements of the sacroiliac joints during standing hip flexion test. Spine 25(3), 364-368
Van Wingerden et al (1993) A functional-anatomical approach to the spine-pelvis mechanism: interaction between the biceps femoris muscle and the sacrotuberous ligament. European Spine Journal, 2, 140-144
Vleeming et al (1989). The sacrotuberous ligament: a conceptual approach to its dynamic role in stabilizing the sacroiliac joint. Clinical Biomechanics, 4, 201-203
Vleeming et al (1989). Load application to the sacrotuberous ligament: influences on sacroiliac joint mechanics. Clinical Biomechanics, 4, 204-209
Vleeming et al (1990). Relation between form and function in the sacroiliac joint. 1. Clinical anatomical aspects. Spine, 15(2), 130-132
Vleeming et al (1990). Relation between form and function in the sacroiliac joint. 2. Biomechnical aspects. Spine, 15(2), 133-136
Vleeming et al (1992). Mobility in the SI-joint in old people: a kinematic and radiological study. Clinical Biomechanics, 7, 170-176
Vleeming et al (1995). The posterior layer of the thoracolumbar fascia: its function in load transfer from spine to legs. Spine, 20, 753-758
Vleeming et al (1996). The function of the long dorsal sacroiliac ligament: its implication for understanding low back pain. Spine, 21, 5, 556-562
For more references see also
Updated : 24/09/2018
 What We do
What We do What We Treat
What We Treat



















































































































