



The development of the concept of musculoskeletal functional stability in the Physiotherapeutic clinical reasoning process by Martin Krause, Dec 2006
B.Appl.Sc (Physio), M.Appl.Sc (Manip.Physio), Grad.Dip.Hlth.Sc(Ex&Sp), Grad.Cert.Hlth.Sc.Edu, Cert IV Workplace Assessment & Training.
Stability is a multi-dimensional concept in musculoskeletal physiotherapy. Essentially, muscular stability involves a spectrum from motor control to immune systems within muscles, Clinical reasoning involves the process of incorporating these concepts into interpreting the clinical presentation and in turn using these principles for the management of the condition.
During my last undergraduate semester at University in 1986 I had an assignment titled "Why don't our shoulders subluxate". At the time the scope of thought was that the supraspinatus was entirely responsible for that stability. Whilst surfing on Cronulla beach I reflected on my problem since I was required to write a 5000 word essay as well as present a 40 minute paper on the topic!
It certainly became clear to me that the previous simplistic dogma wasn't going to be enough to solve the problem. Luckily, we had some inspirational lecturers at the time in the form of Janet Carr and Roberta Shepard. They steered me in the direction of the Russian mathematician Nikolai Bernstein and his seminal work of the 1930's on the motor control problem over the degrees of freedom around the shoulder.
Since that time the Australian Schools of Physiotherapy have considered stability across body parts and addressed the issues of motor control and pain from several different perspectives. These have included
1. The absolute stability of isometric contractions
Generally speaking, this type of stability training is only useful for regions with little movement. An example is the activation of the transverse abdominis and internal oblique muscles in sitting.
![]()
Interestingly, the use of muscle energy techniques employs isometric contractions and mobilization of pelvic and spinal segments for the optimization of muscle control and symmetry across the pelvis.
2. The dynamic stability of rotating systems which use mathematical geometric reference points
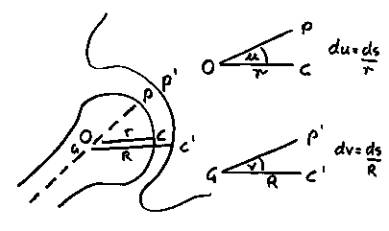
These geometric reference points were emphasized by Saha (1983) in calculations of pure rotation control. However, it was Turvey et al (1978) who proposed that it was the synergistic recruitment of the scapula and glenohumeral muscles which required a controlling mechanism. Turvey et al (1982) who emphasized the recognition of contextual settings as the most important aspect of motor control.
Entropy and Low Back Pain
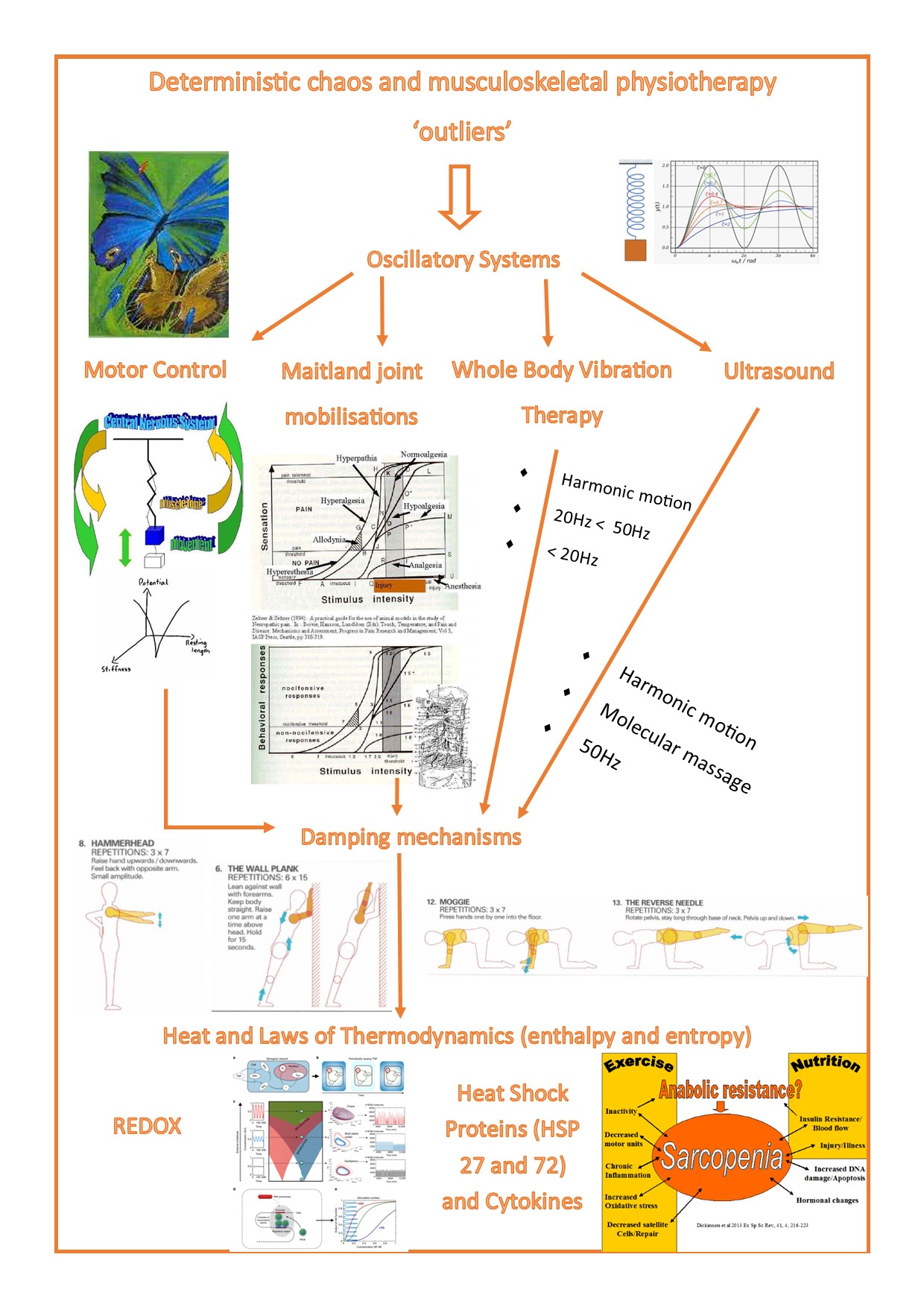
In Musculoskeletal Physiotherapy there has been an emphasis on 'normal'. What is normal function and what are the constraints of a functional movement pattern. Reductionist approaches are taken to ascertain the directions of movement of 'preference' versus those of 'avoidance'. Avoidance in the acute stage of an injury frequently involves 'unloading' the injured area, whereas people with chronically painful movement frequently 'overload' the area of dysfunction. Ironically enough, their movement becomes 'predictable' and less varied. Furthermore, the reduced variability leads to either 'increased control' and less adaptability, or 'reduced control' and increased loading of 'fatiguable structures' (Thiry et al Entropy2022, 24(4), 437; https://doi.org/10.3390/e24040437). Hence, the danger for the physiotherapist is to 'drill' down to the 'offending' structure or movement, but not progress rehabilitation far enough, to include the variety entailed in the full spectrum of complex movement and loading, which is required for motor control in 'predictable' and 'unpredictable' environments. Similar, to the 'Butterfly Effect' in non-linear mathematics, optimisation ultimately requires a chaotic system of control, manifested by 'outliers' which determine the 'damping' or 'amplification' of an oscillating system. Similar, to the 'Butterfly Effect' in non-linear mathematics. Read more : Deterministic Chaos and Musculoskeletal Physiotherapy
3. the dynamic stability of oscillating systems
Turvey et al (1982) suggested that the problem of motor control could be solved by considering the system moving in periodicies which were constrained around a fixed point by the resistance encountered with movement. This hypothesis moved away from peripheral proprioception feeding information back to the brain. Instead we were examining the problem in the context of 'feed forward' systems where proprioceptive feedback' was only required if our objectives weren't met.
Although the original hypothesis pertained to the region of the shoulder, analysis of muscle activity in the abdominal region during arm movements in the mid 1990's by Richardson et al led to some interesting feed forward conclusions involving the transverse abdominus and multifidus muscles.
4. The uncontrolled manifold hypothesis for periodicies
Yet how does learning of feed forward mechanisms occur. It was suggested that releasing and reorganizing degrees of freedom are processes that accompany practice (Schmidt & Lee 1999). Recently an “uncontrolled manifold hypothesis” was proposed which assumes that when a controller of a multi-element system wants to stabilize a particular value of a performance variable, it selects a particular subspace where the desired variable is held constant. Simultaneously, other elements can show a high degree of variability so long as they do not affect the essential variable (Latash et al 2002). Similarly, closed loop theory suggests that a learner acquires a reference of correctness (Schmidt & Lee 1999).
5. The stability of inverse dynamics
With the introduction of force and momentum into the motor control stabilization argument, the natural thing to consider is the effect of Newtons 3rd Law of Action - Reaction. When applied to accelerating body parts which have mass and hence momentum, then the balancing and counterbalancing forces can be calculated and their perturbations can be used to optimize movement. The great thing with this development is that it allows us to consider the parallel and series elastic components as springs providing recoil energy, whilst muscles provide eccentric-concentric energy capturing efficiency by opitmizing the trajectories of moving body parts. Combining these concepts of elastic potential and kinetic energy with inverse dynamics gives some resolution to the problem of control of the 'inverted pendulum' which is walking. Similar to rockets or sedge way systems the propulsive force acts up from the ground resulting in a potentially unstable mechanism. Body perturbations such as swing and pendular movements of the arms help counter these potentially destabilizing forces. Additionally sinusoidal oscillations in the soft tissue acting at a microscopic molecular level up to the level of cytoskeletal and musculoskeletal architecture probably impacting on stability through the dynamic alterations and adjustments afforded by the principles of tensegrity; whereby actin like moelcules are able to change the cellular architecture to adapt to forces developed by vibration and fluid shear.
Plyometric exercise regimes employ concepts of inverse dynamics for the optimisation of movement efficiency. More recently, these type of exercises have also been emphasized for recovery from tendonosis as it benefits both the parallel and series elastic components, as well as blood flow and more importantly the capture of transverse force energy for longitudinal muscle displacement.
During the early 1980's Bergmark described muscles based on their biomechanical characteristics dividing them into two fundamental elements - local stabilisers and global mobilisers. A decade later in the early 1990's, a fundamental development in the concept of stability was from Punjabi where he described elements of control which included the passive elements (ligaments, capsule, etc), the active elements (muscle) and the 'active controller' as an integrated system of satbility. A pain element was later added by Lund et al (1991) whereby they described the inhibition of the agonists and facilitation of the antagonists in a peripheral area of pain.However, in the trunk a different interplay of muscles was construed, whereby Hodges et al (1995) and Hides et al (1994) later suggested that this peripheral motor pattern may be represented by inhibition of the multifidus and transverse abdominis muscle in the trunk. Furthermore, Wim Dankaerts and Peter O'Sullivan (2005) further suggested that facilitation of the gobal mobilisers into stabilisers resulted in motion and/or movement impairment with excessive compression of the spinal vertebrae and their comprising elements leading to reduced postural pertubations and reduced degrees of freedom.
The complexity of spinal control in the presence of pain has lead to many clinical assumptions. Spinal stability involves the co-ordination between several muscles to prevent Euler Buckling of spinal segments. There is strong evidence to suggest that the deep fibres of lumbar multifidus controls spinal motion. Multifidus contributes to 2/3 of the stiffness at the L4/5 (Wilke et al 1995) and in vitro studies (Punjabi et al 1989, Kaigle et al 1995) demonstrate contraction of multifidus increases intervertebral stiffness at an injured lumbar segment. However, it is notable to consider that all lumbar muscles contribute to stability of the lumbar spine (Cholewicki and VanVliet 2002, McGill et al 2003). Co-contraction of the superficial flexors and extensors are required to control intervertebral motion via compression. However, it has been argued that sustained compression could be detrimental to the spine (Nachemson and Moris 1964, in MacDonald, Moseley and Hodges 2006, Manual Therapy, 11, 254-263). Muscle fibre composition has also been considered as important when considering issues of stability where type I endurance fatigue resistant fibres of deeper layered muscles are thought to contribute to tonic postural control. However, fibre composition has generally been exptrapolated from investigations into disuse atrophy and exercise induced hypertrophy and furthermore, specific muscle biopsies of the paraspinal muscles have been done on cadavers or people undergoing spinal surgery (MacDonald et al 2006). Moreover, assumptions have been made that disuse atrophy is the opposite of exercise induced hypertrophy, which may not be the case. Never-the-less, Belavy et al (2007) have demonstrated a tonic-to-phasic shift of lumbo-pelvic muscle activity during 8 weeks of bed rest and at 6 months follow-up with tonic activation of short lumbar extensors and a similar trend for thoracic extensors, with a phasic trend for internal oblique and inferior gluteus maximus (J Appl Physiol, 103, 48-54). However, these results reflected EMG activity rather than muscle biopsy results. Furthermore, the concept that deep multifidus (DMF) is tonically active is not bourne out by the literature. Instead, spatial and temporal features of DMF activation reflect the activity demands of constantly changing internal and external forces on spinal control (MacDonald et al 2006). DMF activity tends to be based on feedforward mechanisms which allows for non-direction specific activity to occur prior to the onset of movement (Moseley et al 2002, 2003). Fear of pain has been demonstrated to reduce the flexion-relaxation phenomenon of paraspinal muscles during forward bending which presumably could alter DMF activity (MacDonald et al 2006). The advantage of the DMF is that it can control shear and torsion without generating a torque and therefore doesn't require a co-contraction from an antagonist to maintain stability. Furthermore, the evidence doesn't support the need for co-contraction of Transverse Abdominis and DMF (MacDonald et al 2006). Clinically DMF atrophy can be seen on MRI in people with chronic LBP. Wallwork et al (Manual Therapy 2009, 14, 496-500) demonstrated patterns of localised MF atrophy in CLBP which also demonstrated reduced ability to voluntarily contract the atrophied muscle during real-time US. Similarly, reduced Tr Abdo activity can be seen during Real Time US, regardless of the ability to contract presumably synergistic muscles such as the pelvic floor musculature. With the burgeoning research into prolonged spaceflight, future bed rest investigations should clarify some of these paradoxes.
6. Vestibular and verbalisation for stability
In the 1970's, Hon.Dr Med Suzanne Klein Vogelbach took a vestibular approach to agonist - antagonist recruitment and hence 'timing' of synergy. In cats, lack of vestubular input has been shown to reduce extensor muscle tone (Magnus 1926 in Belavy et al 2007, J Appl Physiol, 103, 48-54).
Klein Vogelbach also placed a large importance on complex language constructs when assessing and administering exercise for movement dysfunction. Apart from an existential philosophical construct of reality, the manipulation of language seems to underlie concepts of verbalisation for accessing the subconscious in the development of expertise, and is also used in neurolinguistic programming as well as congitive functional therapy.
7. Mental stability such as sporting performance in orienteering
With the evolution of each new concept the emphasis is still placed on higher centre motor control. However, since the brain can only process one piece of information at any one instance, and can only hold 6 pieces on information in short term memory how can this control movement? Indeed for control to occur it must be processed subconsciously, thereby freeing the conscious brain for decision making when the automated processes sense inconsistencies. The most powerful access to our subconscious brain is through our ability to verbilise and visualisel our expectations. Hence, in orienteering, the athlete can read the map to analyse the upcoming terraine thereby preparing their motor system for what will be encountered. Such preparation lends itself to pacing strategies and goal oriented feedback whereby anticipated feedback act like red and green traffic lights. Self affirmation requires little conscious effort e.g. is this the correct track and there is the rock followed by a spur and a clearing with a small gully to my right. If these features don't fit the terraine being scanned by the visual cortext then the greater mental effort of conscious correction and decision making needs to be employed.
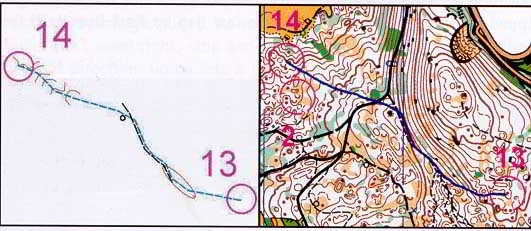
link to motor learning in orienteering
Acquisition of motor control requires context specific variability. Variability is particularly important in orienteering as each course is unique and different. Without variability, injury and/or sub-optimal performance is likely to occur.
8 Neuro-linguistic feedback stability
From Switzerland, the Hon Dr Med Prof Klein Vogelbach (Functional Learning Theory {FBL = Funktionelle Bewegungs Lernen}) used powerful linguistic analysis of visual and tactile inputs to force physiotherapists to communicate their thinking with their clients. Hereby, a 2 way discussion ensued which could be argued lead to a stabilizing relationship between the therapist and their client and with the client and their own condition. This narrative reasoning has been propagated by Mark Jones in Adelaide. More-over the semantics of language and the power of words have been used to ascertain peoples fears and beliefs as they pertain to movement. In fact, Peter O'Sullivan has encouraged therapists not to use the term 'instability' as it may elicit fear-avoidance movement behaviour in people.
Peter O'Sullivan LBP movement classification disorder
Peter O'Sullivan further classified Pelvic Disorders into excessive/lack of force closure or poor form closure. Excessive force closure involves increased muscle activity across the pelvis leading to compression of the SIJ. Lack of force closure results in excessive movement around the SIJ and pubic symphasis which can lead to poor form closure whereby the opposing complimentary irregular surfaces of the ilium and sacrum move into positions of reduced stability such as 'counter-nutation'.
9. Stability through occulomotor reflexes
This form of stability has gained a lot attention through the work on Whiplash injuries by Michelle Stirling and Gwen Jull at the University of Queensland. They advocate the use of powerful visual reflexes to optimise both static stability as well as tracking stability. Additionally, they use pointer devices beamed from peoples heads onto a target on a wall to test and train peoples correctional ability after the eyes are shut, or when the body is turned whilst trying to keep the head stable. This is in line with their revolutionary regime of training deep neck flexors, improving scapula control, reducing muscle spasms and over-activity to improve functional stability.
10. Metabolic and Immune stability
Exercise for musculoskeletal disability has been advocated for both acute and chronic musculoskeletal conditions, yet it involves the paradox of the balance between anabolic and catabolic stressor states which can have profound effects on our immune systems. Over-reaching in daily life and over-training to balance cognitive stressors may be creating more harm than good

Altered biomechnical conditions are a result of misuse, disuse, abuse whose damage causes a reciprocating viscious cycle of muscle-tendon atrophy, degenerative changes, and immune-metabolic dysfunction. At Back in Business Physiotherapy we use a combination of 'hands-on' therapy, exercise and nutritional supplementation to optimise the rehabilitative process. Moreover, endurance is tantamount to musculoskeletal health, as the deeper slow twitch postural muscles are the stabilisers of the body. In contrast the multi-joint superficial muscles are the mobilisers - ballistic muscles of the body. Good training involves building a physiological endurance base with graduated progressive and periodised training regimes.
Immunological factors as a result of disuse
A biphasic stress response has been described in muscles during 'reloading' after a period of 'unloading'. Mechanical unloading as a result of disuse results in substantial muscle atrophy. This atrophy is a result of both increased protein degradation and reduced protein synthesis. Signaling pathways leading to this, include oxidative stress, proinflammatory signaling, reduced stress response, including heat shock proteins (HSP) and insulin-like growth factor (IGF-1). Insufficient HSP and antioxidant enzymes elicits oxidative damage of proteins and lipids (Lawler et al 2003, Free Radic Biol Med, 35, 9-16). Hence, unloading elevates oxidative stress. Paradoxically, loading also elevates oxidative stress. Nuclear Factor kB (NF-kB) has been implicated in both processes. During unloading it is thought to induce numerous pro-inflammatory genes including nitirc oxide synthase, cytokines, ubiquitin pathway ligases as a result of withdrawal of the stress - response including HSP25, HSP70, IGF1/Akt pathway (Lawler et al 2006, Muscle Nerve, 33, 200-207). The early portion of reloading, after a period of immobilisation is characterised by muscle damage and inflammation which requires a cognitive approach using a realistic time-frame for recovery to take place. although, muscle recovery after 7-10 days of unlaoding is rapid (7 - 9 days), prolonged immobilisation greater than 17 days exhibits impaired recovery of muscle mass (Kasper 1995, J Appl Physiol, 79, 607-614). Reloading of muscles have been shown to result in a large up-regulation of NF-kB DNA-binding activity (Lawler et al 2012, Med Sci Sp Ex, 44, 4, 600-609). HSP25 phosphorylation decreased during prolonged unloading but returned to normal after 28 days of reloading. HSP70 and IGF-1 remained depressed during short term reloading but returned to normal levels as muscle mass improved, whereas in contrast Akt phosphorylation was greater in short term reloading but returned to normal by day 28 (Lawler et al 2012).
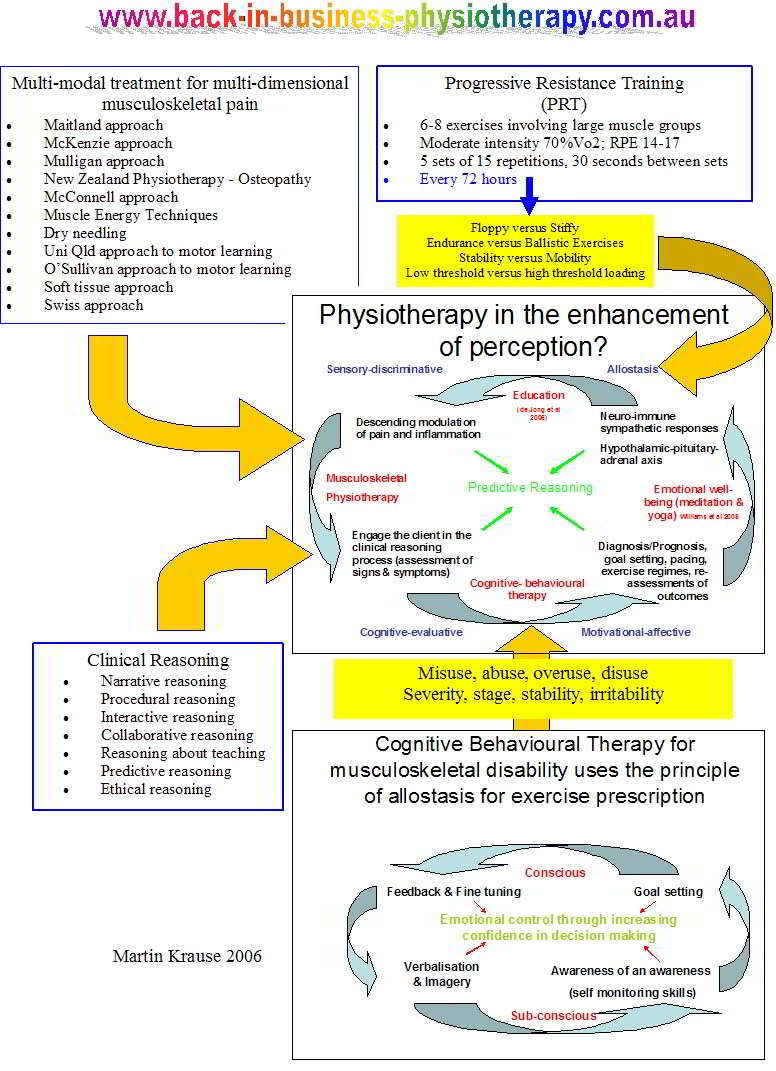
Muscle mass is considered fundamental for the production of force and hence power. I submitted a paper for publication in 2003 which outlined the importance of muscle mass to immune, hormonal and metabolic function. From this paper, the concept of total body stability and allostasis was born, which I presented in Rome in October 2005.
- Muscle mass has been traditionally associated as an organ of movement, however it is an organ of survival and hence allostasis, as it represents 90% of protein in the body and is an important site of both local and systemic immune - inflammatory reactions
- Progressive resistance training (PRT) associated with goal oriented cognitive behavioural therapy (CBT) represents a credible method of mediating the risks of developing sarcopenia and metabolic syndrome as well as improving immune responses to stress and inflammation.
- Periodisation of training represents a credible method of stressing rather than straining the system. Additionally, specific plyometric exercise regimes have the potential to enhance the myofibrillar architecture thereby reducing the amount of trauma and inflammation occurring during weight bearing eccentric exercise regimes
- Nutritional supplementation and adequate time for recuperation will enhance immune responses
- Goal oriented specific task demands within given time frames and associated with appropriately timed feedback (both internal and external cues) will enhance allostasis and hence improve the immune response.
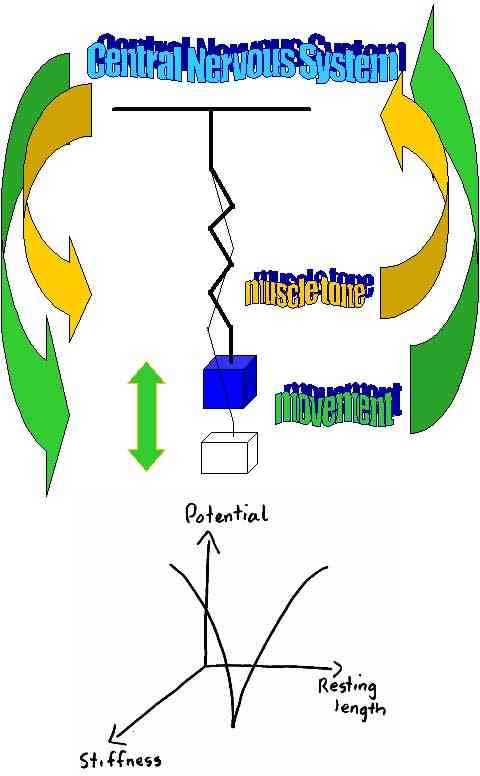
11. Emotional stability
Since the central nervous system and resting muscle tone are particularly important aspects of motor control, then emotional stability is of paramount importance for optimal performance. Extreme examples of mal-adpative behaviour to emotionally labile states are situations which lead to 'fear - avoidance' of activity. Optimisation of the emotional state can lead to the feeling of control over the environment rather than the reverse, "master of their own destiny". Such scenarios also result in large amounts of energy being available which if constrained through 'pacing' can result in athletic success but if unchecked can cause euphoria which ultimately leads to a "crash and burn" phenomenon.
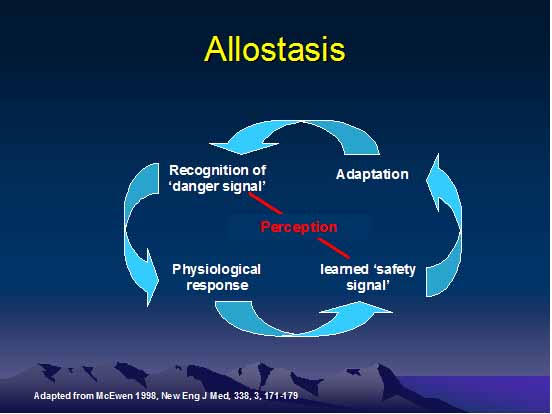
It could be argued that the term 'instability' could lead to 'fear avoidance' behaviour with inappropriate sympathetic nervous system activity. Hence, the concept of allostasis and neuro-immune behavioural mechanisms need to be considered here. Allostasis represents the ability to go beyond ones comfort zone and to adapt postively to the 'stressor' over time.
Negative emotions such as rumination can be ascertained on questioning the client about the intial precipitating incident. Additionally peoples attitude towards them, in the working/sporting, home and social environment may have an impact on the persons 'emotional stability' as well as their ability to cope actively.
12. Clinical stability
Clearly, the gaining of sporting expertise (such as pitching in baseball) can only be obtained through repitition of movement (practice), whilst avoiding injury. Furthermore, when injuries do take place appropriate recovery from injury should occur. Generally, people consider recovery to be synonymous with being painfree. However, over the years we have learned that motor dysfunction can continue in the absence of pain, thus leaving a person vulnerable to further injury.
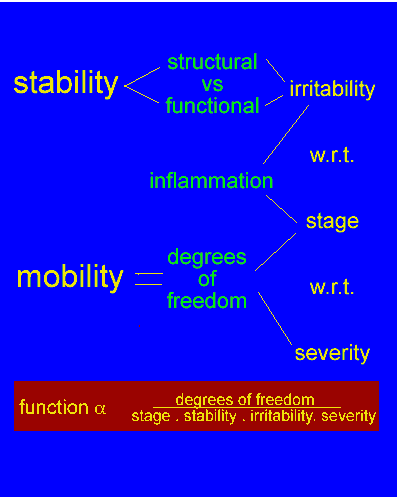
Clinically, the Maitland edition of Peripheral Manipulation from the early 1990's emphasized the concepts of stage, severity,irritability and stability. Unfortunately, these concepts were thought only to apply to joints, which at the time was considered a 'passive structure' (e.g. passive accessory and passive physiological). Yet the concept of 'stability' suggested a clinical past history of questioning the frequency of recurrences. 'Irritability' was emphasized and considered the ease of exacerbation of pain and the time required for it to subside, yet it was meaningless if considered outside the concept of stability. The 'stage' of the problem explained whether a condition was getting better/worse or staying the same, but was only meaningful if the 'severity' of the condition was considered. By examining 'severity' the authors were actually considering today what we would describe as 'avoidance behaviour'. Hence, it was important to know what the person was and wasn't doing. They may appear stable and non - irritable but what had been eliminated out of their activities of daily living? Addressing 'easing factors' can give an indication of whether the person copes 'actively' or 'passively'. Such cognitive evaluation by the client's higher centres is now considered an integral part of the examination and treatment process when determining the motor control issues affecting their musculoskeletal system.
Even despite the knowledge that pain could cause reflexogenic inhibition and excitation of muscle activity, pain was clearly a missing ingredient in many models of motor learning. By 1993, at the Parisian IASP world congress, French researchers had mapped descending noradrenergic modulating pain pathways in rats (Proudfit, H.K. (1992). The behavioural pharmacology of the noradrenergic descending system. In : Besson, J.M. & Guilbaud, G. (Eds.)(1992). Towards the use of Noradrenergic Agonists for the Treatment of Pain (1st ed.). Amsterdam : Elsevier Science Publishers B.V.), whilst the first MRI and PET imaging started to become available and affordable to general patient populations (IASP world congress, Vancouver 1996).
Although the concepts of motor learning, skill acquisition and stability have seemed like a parallel phenomenon to the traditional approach to physiotherapy, this shouldn't be taken for granted. The Swiss physiotherapist and founder of Functional Movement Learning, Honorary Doctor Medicine Klein Vogelbach, used concepts out of neurology, in the 1970's, such as training with Swiss balls and brought them across to musculoskeletal physiotherapy. Other watersheds included, the McConnell technique of 'patella taping' which was actually developed at Sydney University in the mid 1980's and had a strong stabilising motor control emphasis drawing on the works of the Americans Gentile and Sahrmann. By the mid 1990's Hodges, Richardson, Jull et al at the University of Queensland placed emphasis on the stability from the transverse abdominal and multifidus muscles in treating low back pain. Interestingly, Klein Vogelbach had already incorporated small spinal rotational movement training into her Functional Movement Learning (FBL) regime at least a decade previously, presumably to stimulate the small intraspinal muscles. By the late 1990's, Lorrimer Mosely was using techniques out of rehabilitation in Neurology, such as reverse mirrors, to take a revolutionary perspective on motor control and neuropathic pain. Similarly, Peter O'Sullivan from Western Australia drew on work in Neurology and Psychology (CBT) to determine and validate a new classification for the treatment of chronic low back pain which has been termed Cognitivel Movement Therapy.
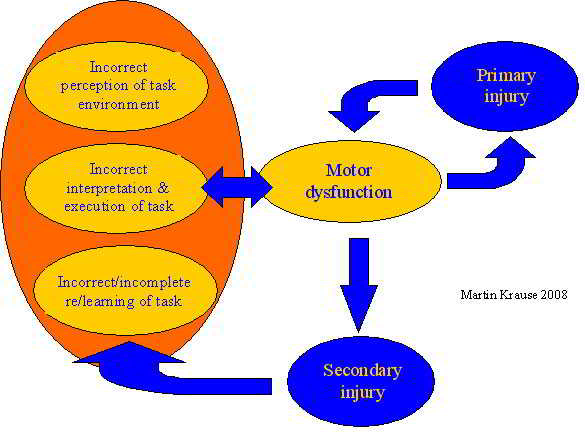
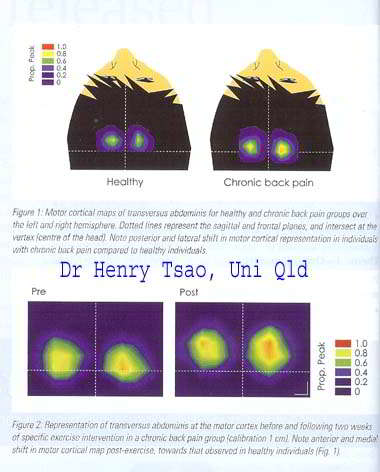
Inconsistent findings on the effects of pain on motor control has made it important to conceptualize a theoretical framework of adaptation in the sensorimotor system in the person with pain. A simplistic approach would be to say that the person will use the redundancy in the system to protect the perceived vulnerability to further injury. Such redundancy takes the form of employing synergistic muscles to perform the task and/or adapting the task to reduce loading. In the acute phase of an injury, such simple strategies may be useful, however adapatation can be very rapid and permanant. If the adaptation is suboptimal for the intended goal, then secondary injuries may occur. These may take the form of disuse atrophy, reduced sensorimotor (proprioceptive and feed-forward) input from the 'unloaded' part, whilst overloading the compensatory muscles and the body parts which they influence. Therefore, both the primary and secondary consequences of the movement dysfunction must be evaluated and treated. Henry Tsao at the University of Queensland has quite clearly shown alterations in cortical processing regions (motor maps) in the brain in people with chronic low back pain. Adaptation strategies vary between people with both increases and decreases in muscle activity occuring in various parts of the body. Thus it becomes imperative that the person is examined in a systematic way in order to specifically taylor treatment management strategies.
Levin et al (2008) mapped the gene expression of pain which in the case of muscle tissue proteins and neural tissue probably has an influence on motor control.
13. Deterministic Chaos and the Immune Muscular Oscillatory system
13. Oscillatory systems and determinstic chaos - immune considerations
We were born from the chaotic fire of genesis. Laws of thermodynamics dictate our existence. Evolution of heat shock proteins (HSP) means that we are our immune system. Today, human multi-cellular life is still totally dependent on our unicellular ancestors and their componentry. Trillions of species and bacteria in the gut (flora) and skin alone, associated with immune substances, attest to the importance of unicellular life in the immune system. The abundance of energy species in the gut suggests a nexus with one of the organs most in need of energy, the skeletal muscle. Importantly, muscle cells have more mitochondria than most other cells, so they can readily produce work for movement. Consequently, muscles are an energy system and an immune endocrine organ. Notably, the development from unicellular to multi-cellular life needed movement. A commonality of cellular movement and macro-muscular movements exist.
Physiotherapeutic and training interventions must consider the health of the immune system and its ability to deploy and be re-deployed. Training should avoid becoming 'stale' by having enough variety (chaos) to create perturbations in the immune system which induce up and down regulation of immune componentry. Physiotherapy should be innovative and creative, whereby the physiotherapist additionally considers immune-cognitive aspects of pain and inflammation, when people seek physiotherapeutic intervention after/during a change in their training regime and/or commencement of unaccustomed exercise, or in the presence of immune compromise.
Read more : Physiotherapy, Exercise, Chaos and the Immune System (during COVID-19)
In the 2 decades since surfing in Cronulla, the approach to musculoskeletal disorders and the concept and scientific verification of stability has undergone significant and fundamental changes due to the dedicated work of physiotherapist researchers validating clinicians insights and practice. Unlike 1986, by 2009 a 5000 word paper and a 40 minute presentation on the topic of 'Why our shoulders don't subluxate' would be pretty easy to fill.
Clinically, the examination process must ascertain the affect of pain and injury on attention and stress and its affects on the interpretation of task demands and hence motor planning. The effects of cortical inhibition, delayed central transmission, reflexogenic motoneuron inhibition on motor planning can lead to an altered internal model of body dynamics. Clinically this may manifest as reduced range of motion, altered reflexes and muscle strength, as well as changed movement goals to protect the body part. The clients perception of their problem is a vital part of a 'top down' approach to assessment and treatment. A 'bottom up' approach views the adaptive mechanisms in terms of altered proprioceptive input resulting in inaccurate motor planning. For this reason combination therapy, using passive modalities such as joint mobilizations, taping, dry needling, soft tissue massage, etc must be accompanied by meaningful and well integrated exercise prescription which takes into account the values and beliefs of the client. Moreover, in some cases the use of 'real' and/or virtual exercise regimes may mean that passive modalities are either unwarranted or contraindicated. Cognitive Behavioral/Movement Therapy may be required to address aspects of 'attention orientation' and 'stress'. Regardless, of the approach taken, the goal should be to educate the client on their condition and how treatment interventions can meet their (positive or negative) expectations.
"It is the thoughts which proceed the action which count
considered thoughts, considered action
decisive thoughts, decisive action
constructed thoughts, constructed action"
Clinical example of muscular synergies
Alec presented with 6/12 history of 'patella tracking disorder' which was exacerbated by a 7/7 very hilly multistage Transprovance MTB race where the technical sections were so difficult that he had to walk down hill a lot. This resulted in the onset of Pains A, B and C. 2/12 ago a 'low level burning pain commenced at night in the calf's and thighs'. A few weeks prior to the onset of of this burning pain he had had a 'nasty cold'. There was also a prior history of a fractured collar bone 2 years previously as well as some I/T chronic neck and upper thoracic pain of at least 10 years duration.
Examination revealed a stiff kyphotic T/S, reduced rotation and lateral flexion. Extension of the lumbar spine produced increased adductor on the right associated with some increased distal hamstring activity as well. Otherwise ROM of the L/S and hips was within normal range. One Leg Standing (OLS) revealed increased adductor and hamstring activity during lateral weight shift as well as anterior ilial rotation on the right associated with increased ITB tension. The right leg also appeared to be longer than the left. Bilateral excessive pro-nation was present. Active SLR revealed a positive left side which improved with anterior compression of the left inferior ribs. Active leg extension (ALE) was positive on the right and left with early onset of hamstrings as well as contraction of the thoracolumbar muscles prior to the onset of thighs movement. Vastus Medialis Oblique (VMO) on the left was normal whereas on the right the Vastus Lateralis (VL) came on prior to VMO.
Hence, in terms of motor control we have the initiation of movement being dominated by global muscles such as
- Thoracic erector spine and Hamstrings prior to gluteus maximus contraction
- Abductors(esp right) prior to and even substituting gluteus medius contraction
- VL prior to VMO
- Lack of inferior-lateral and posterior expansion of the diaphragm, probably resulting in reduced eccentric Psoas Major activity.
- Excessive superficial abdominal muscle activity resulting in reduced thoracic mobility with a consequential enhanced outer sling activity
This pain induced dysfunction or this dysfunction induced pain hypothesis was tested by giving the client a series of motor control innervation exercises whereby synergistic action of deep stabilizers such as Transverse Abdominus, Gluteus Medius and VMO were accompanied by posteriolateral left inferior Diaphragmatic chest expansion. Gluteus Maximus activation over Hamstrings was facilitated through exercises aimed at reducing low thoracic/upper lumbar spine erector spinae activity as well as further facilitating diaphragmatic activity. Exercises to reconstitute the foot arches as well as activate Gluteus Maximus and Transverse Oblique were also given.
Additionally, thoracolumbar dysfunction was addressed with mobility exercises for this region employing serratus anterior and posterior (inferior and superior) activity. The innervation of the diaphragm, as well as the serratus anterior and latissimus dorsi was addressed by providing a Deep Neck Flexor and Low Trapezius exercise, which should in turn have an effect on shoulder and lumbar spine stability.
Muscle Energy Techniques were used for the right anterior ilial rotation (counter nutation). Reduction in muscle spasms of erector spine, quadratures lumborum, and VL is achieved through throracic rib mobilizations, soft tissue massage of the thoracolumbar fascia and dry needling of trigger points. The latter has been demonstrated to act on fascia gliding as well as induce the liberation of pro and anti-inflammatory cytokines of the immune system. See link to Dry Needling for more details. Furthermore, immune considerations and recovery from competition and training took into account calorific deficits by suggesting supplementation with carbohydrate-protein powder, fish oil (EPA and DHA 1000mg), magnesium o rotate, Co Enzyme Q10 and Tumeric.
Hereby, stability is achieved through the appropriate timing and synchronization of various synergistic neuromuscular vectors as well as considering the systems physiology as a whole.
also see : chronic low back pain (central)
neurophysiology of pain (peripheral)
neuro-immune considerations in pain
neuro-immune considerations in sport
Published : December 2006
Updated : 9 April 2022
 What We do
What We do What We Treat
What We Treat



















































































































