



There are 3 common shoulder conditions for which a client presents to physiotherapy which have a biomechanical - motor control basis for both the aetiology and continuation of dysfunction. These include
- 'incarcerated long head of biceps' whereby the biceps tendon slips out of it's inter-tubecular groove and becomes entrapped between the joint surfaces
- subabacromial impingement as a result of bursal thickening, posterior inferior capsule tightness causing superior movement of the humeral head on the glenoid during over shoulder height activities, frequently accompanied by weakness of the external rotators, as well as scapula abduction and downward rotation
- multi and uni- directional instability frequently accompanied by weakness in the subscapularis and increased strength or tightness in the external rotators (infraspinatus and teres minor) in for example anterior instability
These altered biomechanical conditions are a result of misuse, disuse, abuse whose damage causes a reciprocating vicious cycle of muscle-tendon atrophy, degenerative changes, and immune-metabolic dysfunction. At Back in Business Physiotherapy we use a combination of 'hands-on' therapy, exercise and nutritional supplementation to optimise the rehabilitative process.
Immunological factors as a result of disuse
A biphasic stress response has been described in muscles during 'reloading' after a period of 'unloading'. Mechanical unloading as a result of disuse results in substantial muscle atrophy. This atrophy is a result of both increased protein degradation and reduced protein synthesis. Signalling pathways leading to this, include oxidative stress, proinflammatory signalling, reduced stress response, including heat shock proteins (HSP) and insulin-like growth factor (IGF-1). Insufficient HSP and antioxidant enzymes elicits oxidative damage of proteins and lipids (Lawler et al 2003, Free Radic Biol Med, 35, 9-16). Hence, unloading elevates oxidative stress. Paradoxically, loading also elevates oxidative stress. Nuclear Factor kB (NF-kB) has been implicated in both processes. During unloading it is thought to induce numerous pro-inflammatory genes including nitric oxide synthase, cytokines, ubiquitin pathway ligases as a result of withdrawal of the stress - response including HSP25, HSP70, IGF1/Akt pathway (Lawler et al 2006, Muscle Nerve, 33, 200-207). The early portion of reloading, after a period of immobilisation is characterised by muscle damage and inflammation which requires a cognitive approach using a realistic time-frame for recovery to take place. although, muscle recovery after 7-10 days of unloading is rapid (7 - 9 days), prolonged immobilisation greater than 17 days exhibits impaired recovery of muscle mass (Kasper 1995, J Appl Physiol, 79, 607-614). Reloading of muscles have been shown to result in a large up-regulation of NF-kB DNA-binding activity (Lawler et al 2012, Med Sci Sp Ex, 44, 4, 600-609). HSP25 phosphorylation decreased during prolonged unloading but returned to normal after 28 days of reloading. HSP70 and IGF-1 remained depressed during short term reloading but returned to normal levels as muscle mass improved, whereas in contrast Akt phosphorylation was greater in short term reloading but returned to normal by day 28 (Lawler et al 2012).
Joint stability in the shoulder
- biomechanics and gamma reflexes
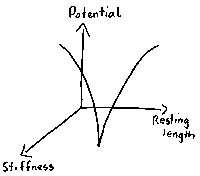 |
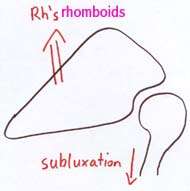
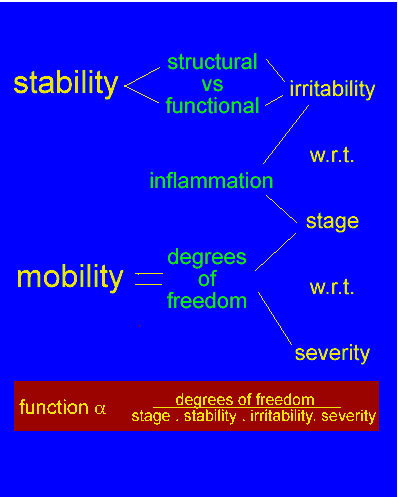
Joint stability is determined by the muscular stiffness in 'soft' joints such as the neck knee and shoulder. Muscular tension generates stability at the glenohumeral joint the outward curves represent the stabilising influence when the prime mover muscles act on the shoulder |
|
|
|
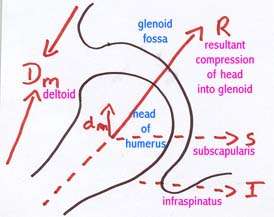
To enable stability at the glenohumeral joint during arm elevation the scapula muscles position the glenoid to provide optimal orientation for the rotator cuff stabilising function |
|
|
If the rotator cuff and scapular muscles do not operate synergistically then the potential for glenohumeral subluxation & subacromial impingement is generated |
|
|
Thorax and shoulder pain
Patients frequently seek treatment for pain in various parts of the body, but infrequently present for treatment of thoracic pain. Yet, simple, quick assessment and correction of the thoracic rings frequently demonstrates a link to the pain and musculoskeletal dysfunction in areas some distance away. Wainner et al (J orthop Sports Phys Ther, 2007; 37, 658-660) describe regional interdependence as “the concept that seemingly unrelated impairments in a remote anatomical region may contribute to, or be associated with, the patient’s primary complaint.” This perception suggests that interventions targeting adjacent anatomical areas may directly affect the outcomes of the involved joint. Boyles et al (Manual Therapy, 2009 Aug;14(4):375-80) and Strunce et al (J Man Manip Ther, 2009, 17(4): 230-236) have demonstrated the immediate effects of thoracic spine thrust manipulation on patients with shoulder impingement syndrome. The latter describing a 51% reduction in shoulder pain, 30-38 degree increase in range of motion (ROM), and a mean patient perceived global rating change of 4.2 in 21 subjects. McCormack (J Man Manip Ther., 2012 Feb;20(1):28-34) showed a 25 degree improvement in shoulder ROM when using thoracic spine manipulation in the treatment of adhesive capsulitis. Brian Mulligan described 'mobilisation with movement' (MWM) techniques on the first rib which have dramatic effects on the cervical ROM for contralateral lateral flexion and ipsilateral rotation. Canadian physiotherapist Linda Joy Lee has advocated ring shift corrections for low back pain, pelvic girdle pain and hip problems, as well as shoulder and neck issues.
Interested readers should look at the thorax aspect of this website.
Summary
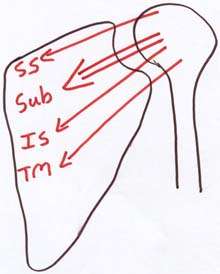
- the rotator cuff muscles provide glenohumeral stability
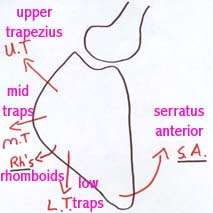
- the scapular muscles provide the positioning for inferior stability of the glenoid labrum for a snug fitting humeral head
- with the deep joint stabilizing muscles providing the stability, the prime movers may provide the 'action'
- generally speaking the stabilizing muscles of most joints are one joint muscles with an endurance function; whereas the prime movers are the muscles which lend power to the movement e.g. Pectoralis Major. Therefore when designing an exercise regime the client must begin with good muscular stability before commencement of training of the prime movers.
- Frequently, clients compensate for lack of stability by increasing the speed at which they do the task. This then leads to further in-coordination, poor timing between muscles, loss of synergy, and more dysfunction.
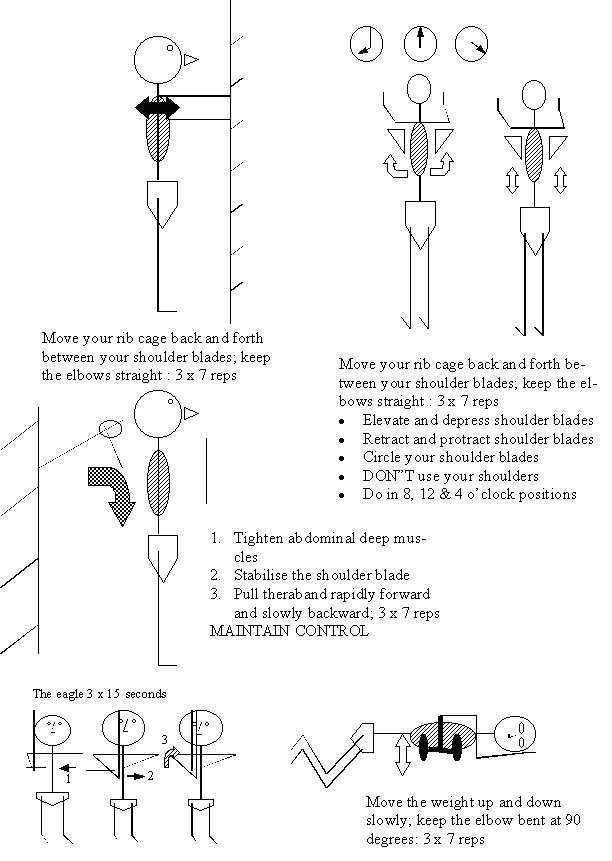
- Closed kinetic chain training to gain scapula and rotator cuff stability may encourage gamma afferent feedback from the annulospiral endings, as well as activate the nuclear bag and nuclear chain fibres
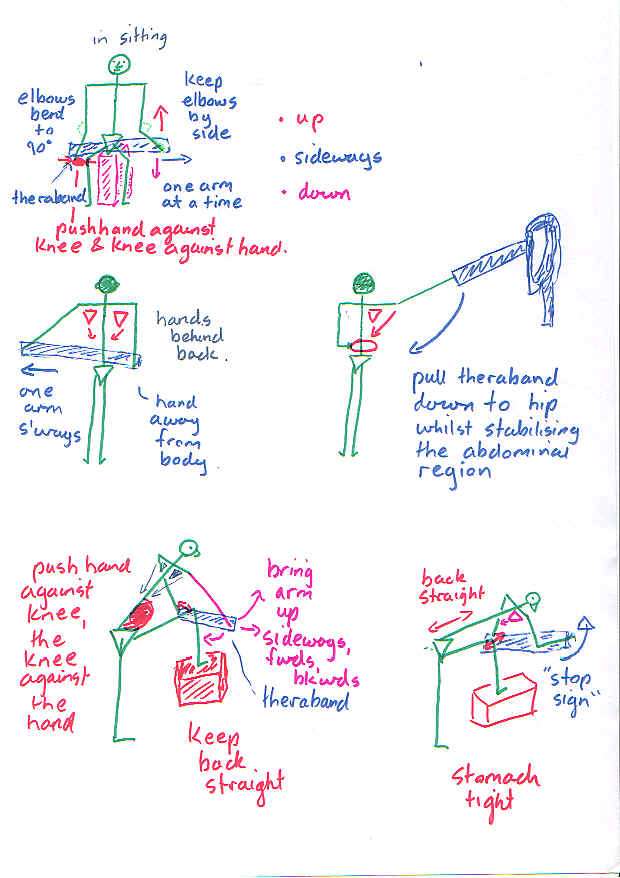
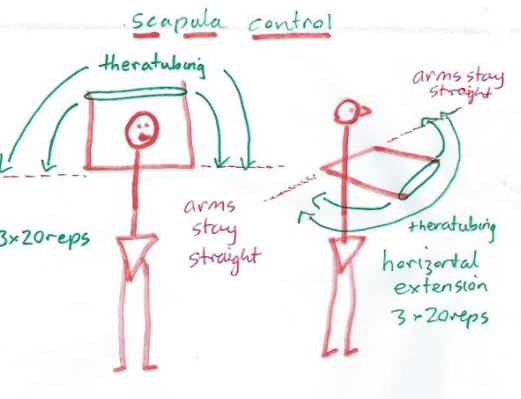
- Plyometric type exercises using theraband are designed to encourage eccentric-concentric control of the prime movers.
Oscillations in another part of the body can be used to establish harmonic frequency elsewhere. For example, arm movements activating the opposite erector spinae activity, pelvic oscillations for scapular control, arm lifts for contra-lateral gluteal activity.

Alternate kneading of the hands into something soft activates the abdominal muscles, spinal rotatores and scapula muscles. Oscillations of the pelvis around the hip activates eccentric scapula control.
Alternate lifting of the arm off the wall activates the opposite buttock muscle.

Alternating arm flexion/extension around the 90 degree angle activates the opposite erector spinae muscles of the low thorax and upper lumbar spine. Moving through the horizontal with a consistent oscillation also has varying effects on those muscles.
Importantly, if loading is required to activate a muscle building response, then repetitions need to include tremor. Either fine motor tremor or exhaustion tremor, if we want to include a 'deterministic chaotic variable', which it is hypothesised to create an immune training variable. Interested readers, on chaos, should view https://www.back-in-business-physiotherapy.com/health-advocacy/exercise-and-the-immune-system-during-covid-19.html
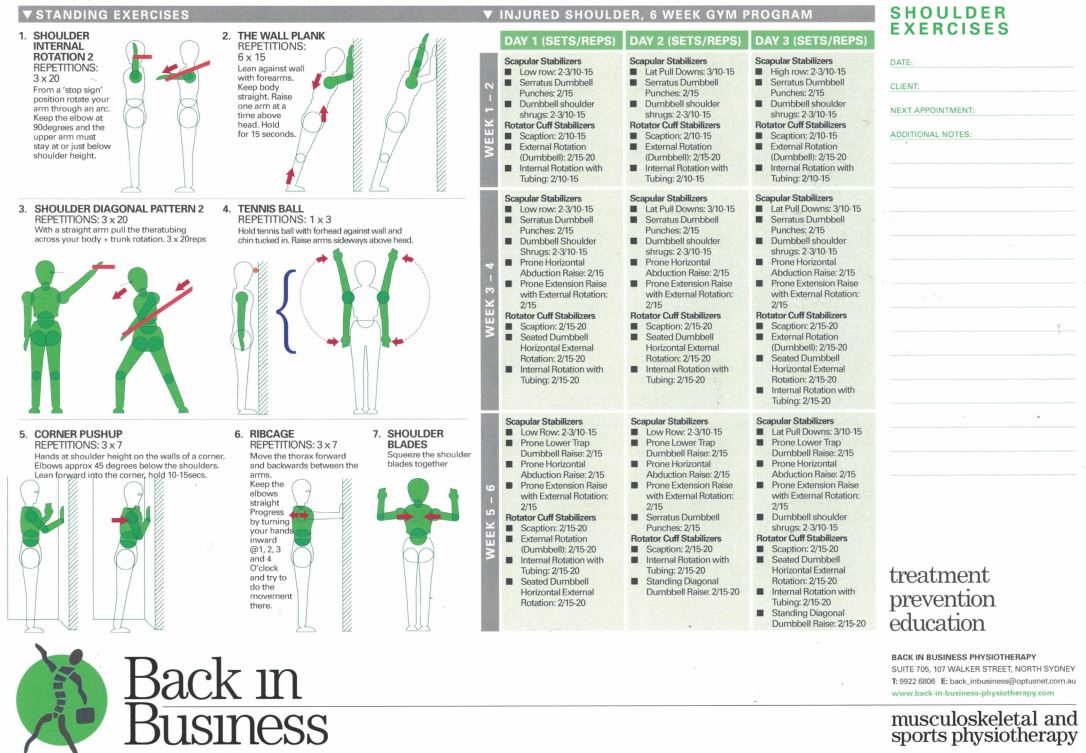
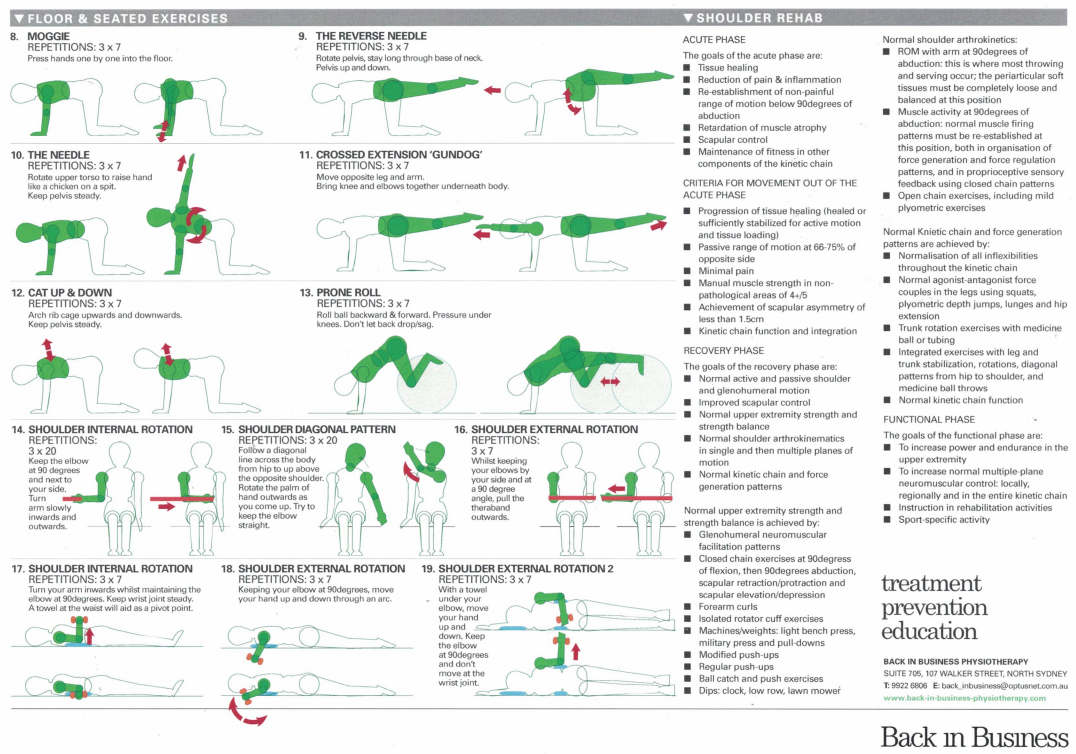
Closed kinetic chain exercises 5, 8-13, promoting stability. Should be done slowly, as the deep stabilising muscles are red slow twitch muscle fibres. Such exercises combine the shoulder, neck, shoulder blade, thorax and pelvic complex to functionally stabilizing activities. Moreover, Swiss Ball Exercises in 2 and 4 point Kneeling can be used to promote over-shoulder-height arm activity whilst having the arms below the shoulders!!! Apart from the Prone Roll, the Swiss Ball can also be used to do diagonal upward rolls as well as prone scissors. Open chain dynamic exercises can eventually be incorporated whilst kneeling on the Swiss Ball
Plyometrics - open kinetic chain
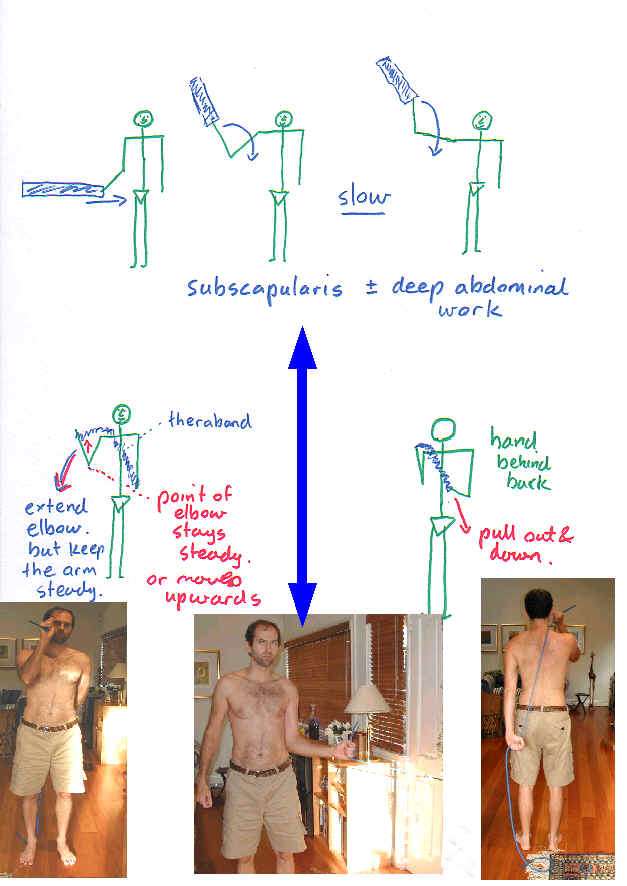
Open kinetic chain exercises are essentially less stable than closed kinetic chain exercises. They fall into two essential categories - those which pull inward and hence energy towards to body and those wish pull away. Basically, hypermobile people need to focus on stability, perfecting closed kinetic chain exercises, moving on to a hybrid of closed kinetic chain with open kinetic chain pulling inwards and eventually adding the open kinetic chain pulling outwards.
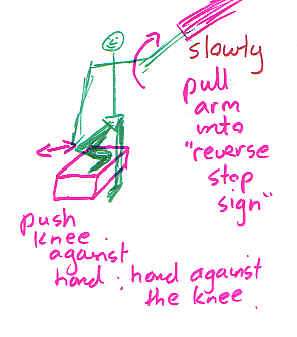
Simply sqeezing the buttocks whilst doing these exercises will activate the deep abdominal core. Additionally, making oneself 'long through the base of the skull', will activate deep abdominal core, encourage diaphragmatic breathing and 'widen' the shoulder blades on the thorax, allowing for better arm swing.
Care needs to be taken with the open kinetic chain internal and external rotation as it's not uncommon to aggravate the transverse ligament and long head of biceps with this exercise. Additionally it isn't a very functional exercise. Exercises that more closely mimic the activity to which the person needs to return to, will generally be more effective, as well as present an opportunity to use the exercise as a metric on the path to recovery.

EMG biofeedback
Altered immune responses and altered lipid metabolism have been implicated as a causative factor in shoulder tendinopathies. Interested readers should look at Exercise and the Immune System as well as Exercise and Weight Loss elsewhere on this website for further explanations.
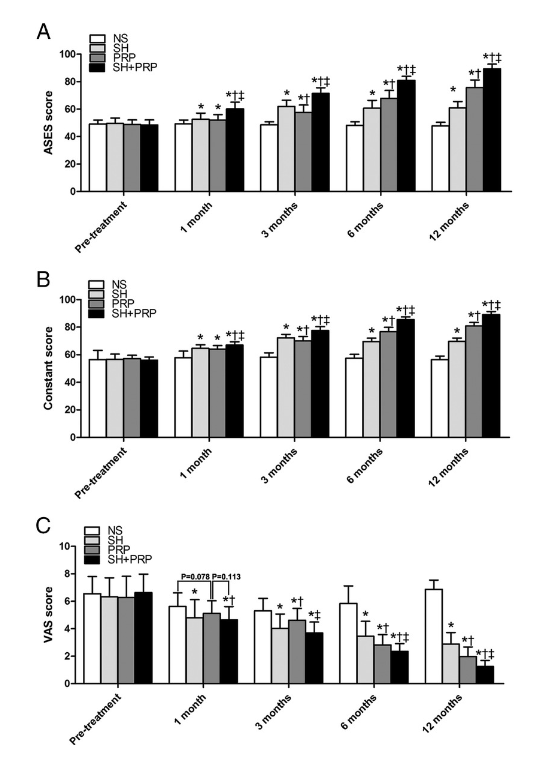
Sodium Hyaluronate and Platlet Rich Plasma (PRP) for partial thickness rotator cuff tears
Investigations have demonstrated improvements in pain and function, in small to medium sized supraspinatus tendon tears, up to 12 months after PRP and Sodium Hyaluronate injections, in 45 people who received PRP injections and 48 people who had a combination of sodium hyaluronate and PRP injections (Cai et al 2019, Med sc Sp Ex, 51, 2, 227-233).
Interesting articles
these articles are particularly interesting in respect to synergistic 'timing' of muscle action in the upper and lower limbs
Commerford & Mottram (2001). Functional stability re-training: principles and strategies for managing mechanical dyfunction. Manual Therapy, 6,1, 3-14
Commerford & Mottram (2001). Movement and stability dysfunction - contemporary developments. Manual Therapy, 6,1, 15-26
Animated muscular synergistic interaction for shoulder abduction - refer to Climbing section
Shoulder Problems(English)
Schulter Probleme (Deutsch)
Last update : 4 November 2021
Last update : 26 November 2013
 What We do
What We do What We Treat
What We Treat



















































































































