



integration and progession of the clinical reasoning process

The Bernstein perspective of functional stability suggests that the body regulates it's movement by using a stable reference of control. This reference of control may be the summation of the muscle tension and neural input around the joint (see shoulder for an example ). Additional input comes from the visual and vestibular systems. Normally, the central nervous system uses feed-forward mechanisms of control whereby descending electrical input on the spinal cord neurones interacts with afferent input from the periphery. This afferent input comes from the nuclear bag and nuclear chain fibres concomitant firing with annulospiral endings providing gamma afferent feedback. Moreover, the movement controller appears to be capturing the momentum of oscillating body segments.
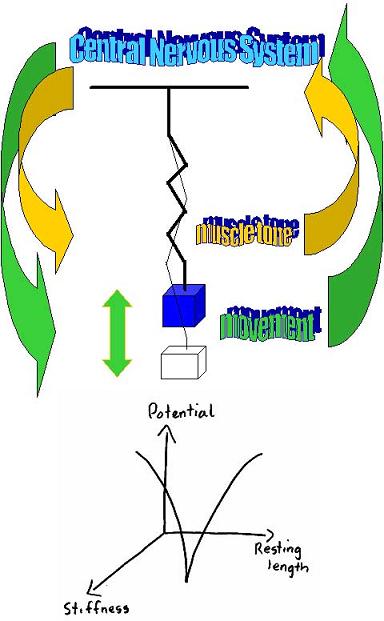
In the presence of pressure on nerve fibres, inflammation and/or pain the afferent input changes resulting in muscle spasms, weakness, loss of co-ordination and reduced proprioception (see Neurophysiology section for more details ). Additionally, efferent firing from the peripheral sympathetic nervous system can change muscle tone as well as blood flow. Finally, cognitive factors such as emotion and fear-avoidance behaviour will influence peripheral muscle tension. Taken together, the functional stability of the system may be compromised leading to excessive stiffness (force closure) or excessive movement.

Either scenario will lead to inefficient use of energy creating unwanted movements in other parts of the body. The laws of inverse dynamics dictate that accelerating body parts will have equal but opposite reactive forces placed upon them resulting in the transfer of energy across the kinetic chain (e.g. foot-knee-hip-back). Therefore, pain and inflammation creates suboptimal biomechanics which can lead to further inflammation and pain in additional areas where these unwanted forces have been directed. For example tight hamstrings &/or early hamstring contraction concomitant with late relaxation of rectus femoris &/or tight rectus femoris can result in counter-nutation and shear across the sacroiliac joint and lumbar spine. This is important as form closure and force closure biomechanics suggest that the pelvis is only stable when the sacrum is nutated. Additionally, tightness of the piriformis creating contralateral SIJ pain due to torsion of the sacrum can also occur. In the former case the client will present with difficulty moving in the saggital plane. In the latter case the client will have problems with unilateral weight bearing. These scenarios can lead to severe intractable pelvic girdle pain, which will require muscle energy techniques and appropriate functional exercises to treat.
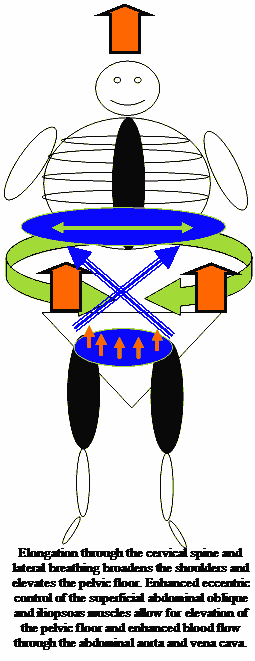
The gluteal muscles of the stance leg requires counter-stability by the contralateral latissimus dorsi and erector spinae (Newtons 3rd law). The attachment of the latissimus dorsi to the transverse abdominis may lead to additional stability. The rotation of the pelvis, being controlled by the stance hip rotators (iliacus, piriformis, obturators) and gluteus medius are countered by the internal oblique and opposite adductor longus. Hereby, rhythmic oscillation of body parts capturing and releasing momentum leads to efficient motion.
The inferior gluteus maximus is used during running and fast walking to bring the foot down onto the ground just prior to stance. Clinically, the inferior gluteus maximus is frequently atrophied whereas the superior gluteus maximus is hypertrophied and tight. The hamstrings may be 'misused' to pull the body forward across the foot. This may result in excessive posterior pelvic tilt, which may make a person appear to be 'sitting down' whilst running. When the hamstring pull is unilateral then a shear force of the ilium on the sacrum may occur. The hamstring muscles are often short and weak suggesting that stretching would result in some instability of their 'energy strap' function. Moreover, during the transition from eccentric to concentric contraction if a muscle is too short then inefficient use of it's elastic recoil potential energy occurs. Therefore the muscle may need to be long and strong in a functionally specific manner.
The Iliopsoas muscle is used to pull the body forward over the stance leg during fast running. The Psoas Major has a different timing of contraction to the Iliacus during jogging compared with walking suggesting that the Iliacus acts as a stabiliser during slower activity. Evidence exists to suggest that the medial aspect of the Psoas major may have a stabilising function whilst the lateral aspect may have a predominant mobilising role. Additionally, the Iliacus may be synergistically contracting with the lateral rotators of the hip to attain this stability. Therefore, low threshold loading of slow twitch endurance muscles function to stabilise joint segments whereas, the laws of 'inverse dynamics' suggest that, the superficial 2-joint high threshold fast twitch glycolytic muscles act as 'energy straps' transferring forces from one body segment to the next (Power = force x velocity). Since the rectus femoris is the only quadriceps muscle which crosses both the knee and hip then it can also act as an 'energy strap'. Importantly, if the muscle becomes short it may lose some of it's potential recoil energy during the transition from eccentric to concentric contraction ( see foot orthotics elsewhere on this site for an example ).
Any stiffness in the rectus femoris muscle can create anterior tilting of the ilium resulting in shear across the sacroiliac joint, as well as potentially creating excessive extension and rotation in the spine. The deep stabilising muscles of the spine and abdominal region will have to work exceptionally hard to prevent excessive and unwanted movement. Thereby, inefficiency in running and walking economy may occur (see running section for further details ).
Notably, the larger muscle groups can have differing functions. For example, the gluteus medius has an anterior, middle and posterior aspect and therefore can create vectorial forces from each of these directions. Additionally, at least 2/3rds of a muscle's longitudinal tension can be dissipated in the muscle's horizontal direction. Finally, it must be emphasised that most muscles have a glycolytic and oxidative capacity whose proportions are genetically determined, but whose transitional fibres can mutate depending upon the type of metabolic demand the exercise prescription entails. Taken together, it is highly likely that the most effective exercise prescription is functionally specific to the goals of the task which is being rehabilitated.
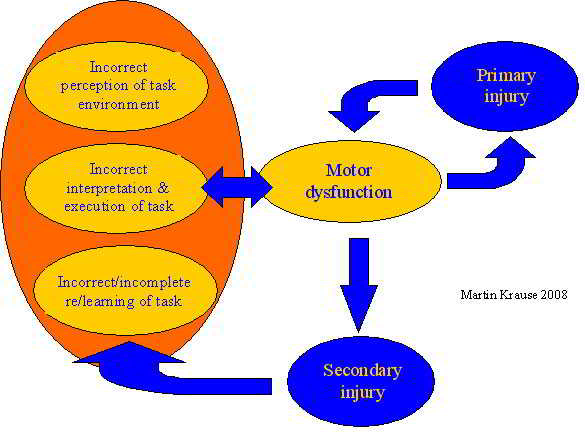
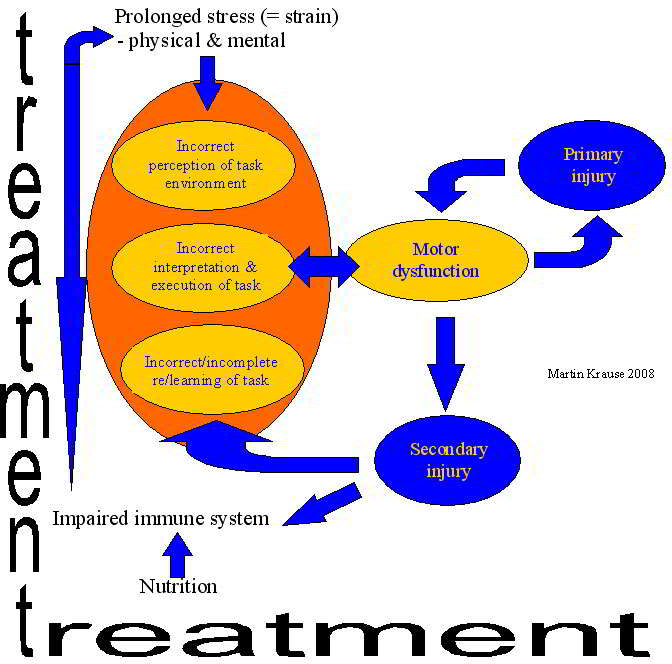
The brain can filter as well as amplify incoming information (see musculoskeletal neurophysiology section ). Cognitive behavioural therapy uses goal setting and feedback to favourably access the central nervous system towards goal specific movement. Expertise in sport is obtained through repetitive practice and the avoidance of injury. Where injury does take place appropriate recovery must follow. Often recovery was considered synonymous with being painfree. However, many recurrent conditions have been shown to be the result of ongoing motor dysfunction.
Examples of gaining expertise and avoidance of injury using higher level motor programming and feed-forward mechanisms to evaluate relevant information
is discussed in the Orienteering section of this website .
This email address is being protected from spambots. You need JavaScript enabled to view it.
 What We do
What We do What We Treat
What We Treat



















































































































