



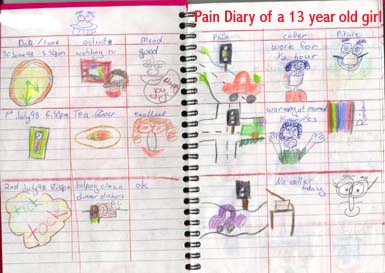
Physiotherapeutic implications of psychometric analysis in the clinical reasoning processThe subjective examination is considered important for assessing the multiple dimensions of pain. A pain diary may be a useful tool to assess the degree of disability in addition to establishing treatment outcomes.
|
|
|
|
|
|
Other psychometric tools for measuring pain include the Vernon-Moir scale, Oswestry, McGill pain questionnaire, Roland-Morris, and VAS scales. These tools are useful for your clinical reasoning process as they establish baselines on which to measure treatment outcome. Moreover, they aid the physiotherapist in the clarification of yellow, blue, orange and black flags. Similarly, they aid the client in making sense of what is happening to them and hence becomes an integral part of the educational process of rehabilitation. General musculoskeletal conditions and pyschometric analysis Do you remember how much you used to have to concentrate when you learnt to drive? Eventually, the task became automated and effortless. However, what happens when you are in an unfamiliar area, you need to look at a map, there is lots of traffic and the mobile phone rings because you are running late for the meeting that you have to chair? Your cognitive systems are bombarded with competing information trying to make itself the priority in your limited processing systems. Similar to RAM in those old computers which couldn't keep up with newer and better software programmes, everything starts to slow and grind to a halt. Back pain can have similar effects on your processing capacity. With constant cognitive hyper-vigilance, a person in pain can have their RAM slow because they have less redundancy to cope with new stimuli. The glutamate-NMDA receptors of the prefrontal cortex and noradrenergic receptors of the locus coereleus may be viewed as the RAM of pain processing. The locus coereleus in particular has been considered an integrator of cerebral activity, helping maintain 'neural synchrony' like a conductor of an orchestra. However these nuclei can undergo neurocytotoxic effects in the presence of excessive and ambiguous interoceptive and exteroceptive inputs. This, may reduce the ability to cope with fear and anxiety in the amygdala and limbic systems. Furthermore, the anterior cingulate gyrus may have it's memory for pain and disability amplified. Connections with the hypothalamic-pituitary axis can result in hormonal imbalance. It is probable that interoceptive bombardment of the CNS by inflamed peripheral nociceptors may be reduced through musculoskeletal physiotherapy hands-on techniques designed to reduce pain and muscle spasm. Additionally, clear explanations by the physiotherapist and structured goal oriented exercise regimes may filter exteroceptive information and thereby clarify 'feed-forward' mechanisms.
Fear connotes an identifiable threat (eg King Brown snake), whereas anxiety connotes the possibility of threat. Fear-avoidance relates to the behaviour that an identified activity may have (real or imaginary). Kinesiophobia refers to the patient experiencing "an excessive, irrational, and debilitating fear of physical movement and activity resulting from a feeling of vulnerability to painful injury or reinjury" (Kori SH et al Pain Management 1990; Jan/Feb:35-43) Avoidance behaviours occur in anticipation of pain and generally persist because there are few opportunities to correct the eroneous expectations which drive them. This has a deliterious effect in the engagement of ADL which then in turn can lead to mood disturbances, irritability, frustration and depression. The fear-avoidance behaviour leads to secondary consequences of deconditioning whereby normal activity such as carrying the shopping leads to excessive fatigue, heart palpitations, nausea and distress.
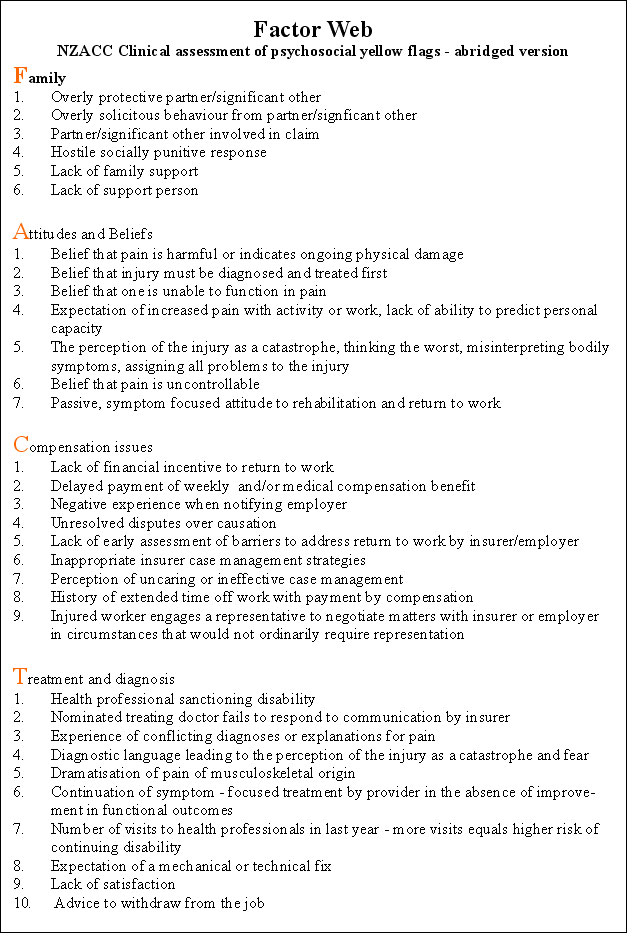
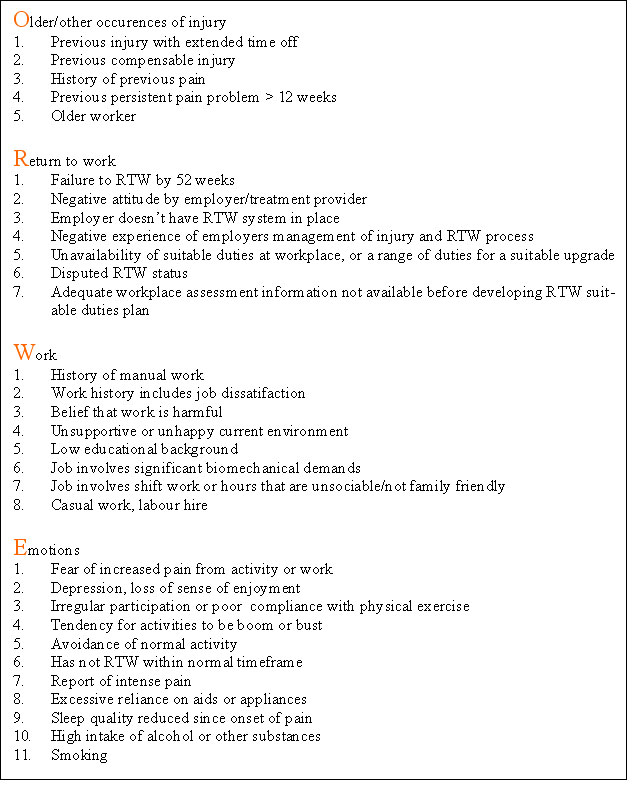
Factor Web
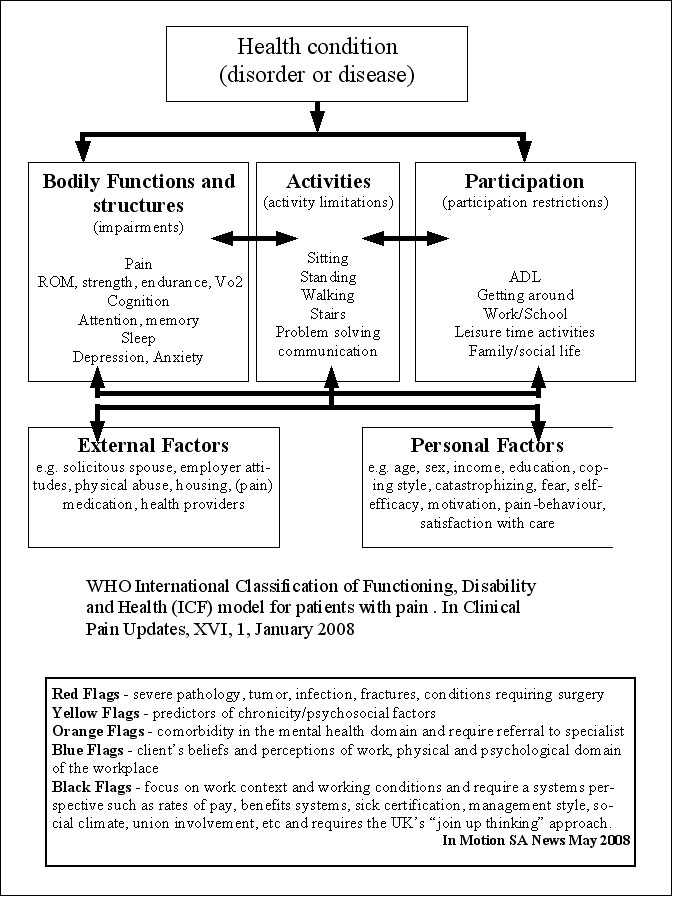
WHO classification of pain
Hewitt, Hush, Martin, Herbert & Latimer (2007), AJP, 53, 269-276, established that measures of activity limitation and pain at 9 weeks, and work status at 6 months have the greatest predictive accuracy of somone developing chronic pain and disability. Psychometric evaluation It is easy to be overwhelmed by such multiple factors which could contribute to chronic LBP. However, we must evaluate what is relevant and use this differentiation to determine what our strengths and weaknesses are as a profession and when to refer to other professionals. Importantly, there will be a significant subgroup of clients who have chronic musculoskeletal injuries due to mismanagement, which if identified could be resolved through multi-factorial physiotherapy which includes passive techniques, exercises and education. The ICF - WHO has stipulated three seperate but related dimensions of functioning are defined as body dimension (functions and structure), individual dimension (activity), and social dimension (participation). Body functions are physiological or psychological functions of body systems. Activity describes daily purposeful integrated body systems execution of tasks. Whereas participation deals with the experiential and contextual setting of the persons life (social relationships, employment, and economic life), as well as societies response to the person's level of functioning. According to Thonnard & Penta (2007), Eur Medicophys, 43, 525-541, "rehabilitation can be defined as a reiterative problem solving and educational process that focuses on disability (altered activities) and aims to maximise participation in society while minimising the stress on and distress of the patient and family". While the outcome of a particular physiotherapeutic intervention can be stipulated based on functional measures, these need to be validated not only w.r.t diagnosis but also their meaning w.r.t the participation of the patient in the community. The latter hasn't specifically been addressed and has frequently been assumed to correlate with functional status. Importantly, functioning and participation in the community are highly likely to be key measures when it comes to financing treatment interventions. Modified Schober Test (MMST) tests range of movement in the lumbar spine in the ICF dimension of body function. Validity as correlated to X-ray is 0.67, reliability as an inter-rater score is excellent (ICC=0.95, 95%CI, 0.44-0.84), responsiveness (sensitivity) requires a change of over 1cm to be 95% confident of change. Thonnard & Penta (2007), Eur Medicophys, 43, 525-541 Low Back SF-36 tests both ICF dimensions of body functions and activities. 18 items pooled from the Australian low back SF-36, modified version of Oswestry and Quebec back pain disability scale has fewer misfitting items than the original SF-36 and thus elimates it's floor and ceiling effects. Unidimensional linear scale developed with the Rasch partial credit model. Inter-rate reliability were 0.94. The minimal detectable change is 12 points on a 100 point scale. Thonnard & Penta (2007), Eur Medicophys, 43, 525-541 Physical Impairment Index (PII) evaluates physical impairment in LBP through 7 tests, each scored dichotomously based on published cut-offs. ICF dimension of body function and structure. Convergent validity was supported by correlations with disability (r=51 w.r.t. Roland Morris Q'naire), work loss in past year (r=0.43), pain (r=0.27), depression (r=0.26 with Zhung depression inventory), somatisation (r=0.32 with modified somatic perception Q'naire), non-organic signs (r=0.49) and non-organic symptoms (r=0.35). Correlations were also found with the physical component of the SF-36 (r=0.28) and physical activity subscale of the fear-avoidance beliefs questionnaire (r=0.24). Good to excellent reliability for individual items (ICC from 0.48-0.96). The overall score demonstrated excellent inter-rater reliability (ICC=0.89) Thonnard & Penta (2007), Eur Medicophys, 43, 525-541 Roland Morris Questionnaire (RMQ) self administered disability measures in LBP reflecting 24 activities of daily living. ICF dimension of activities. The responsiveness is sufficient to detect change after 4 to 6 weeks of physiotherapy in patients with an initial score in the central portion. However, the magnitude of error is too large to detect improvements in patients with a score of less than 4 and deterioration in patients with scores of greater than 20. Thonnard & Penta (2007), Eur Medicophys, 43, 525-541 Sickness Impact profile (SIP) is a behaviourally based measure of perceived health status applicable across a spectrum of illnesses and among various demographic and cultural subgroups, applied in LBP with an ICF participation dimension. Validity has been reported with various biological and clinical measures and subcategories of the Minnesota Multiphasic Personality Inventory. High test-retest reliability coefficient (r=0.85) in LBP. Thonnard & Penta (2007), Eur Medicophys, 43, 525-541 Chronic Pain : Global Physiotherapy Examination 52 (GPE-52) is clinical physical examination in 5 domains including posture, respiration, movement, muscle and skin palpation. Good to excellent inter-rater reliability of the total score (ICC=0.91), and individual components (ICC=0.65 for posture, 0.60 for respiration, 0.89 for movement, 0.83 for muscle palpation, 0.76 for skin palpation). However, requires 3 days of training and some 30 minutes to complete. Thonnard & Penta (2007), Eur Medicophys, 43, 525-541 Orebro Musculoskeletal Pain Questionnaire (OMPQ) is a "yellow flag" screening tool that predicts long-term disability and failure to RTW when completed over 4 to 12 weeks following soft tissue injury. A cut off score of 105 has been found to predict those who will recover (95% accuracy), those who will have further sick leave in the next 6 months (81% accuracy), and those who will have long term sick leave (67% accuracy). In workers with back injuries, at 4-12 weeks, a cut-off score of 130 correctly predicted 86% of those who failed to RTW. The Impact of Event Scale (IES) was developed to measure current subjective distress related to a specific life event (Horowitz M et al 1979, Psychosom Med 41, 209-218).Two response states, avoidance and intrusion are measured. The IES has 15 items, seven of which are intrusive symptoms such as thoughts, nightmares, feelings, and images associated with a specific event. Five of these measure intrusive symptoms whilst awake, wheras 2 others measure intrusions at night (insomnia, nightmares). The avoidance subscale has eight items such as a numbing of responsiveness, and avoidance of feelings and situations. A cut-off of 26 or above would be grounds for a psychological referral. However, a few weeks may be allowed to pass as to allow some natural recovery. Has been recommended by Dr Michelle Sterling in some people who have suffered a whiplash type injury. The Pain Self Efficacy Questionnaire (PSEQ) ask clients to rate how confidently they can perform the activities despite their pain. It covers a range of functions including household chores, socialising, work as well as coping with pain without medication. It is based on Bandura's (1977) conceptualisation of self-efficacy as a reflection of a resilient self-belief system' in the face of obstacles. Takes 2 minutes to complete. Low scores 40 suggest that the client is likely to respond well to an exercise regime. Low PSEQ is a predictor of long term disability and depression. The Pain Anxiety Symptoms Scale (PASS) validity has been supported by positive correlations with measures of anxiety, cognitive errors, depression, and disbaility. Fear of Work Related Activity = Fear - Avoidance Beliefs Questionnaire (FABQ) has 2 parts, one on physical activity, the other on work. The latter has been shown to have significant predictive validity with disability in ADL and days off work, more so than biomedical parameters such as anatomical pattern of pain, temporal pattern, and pain intensity. Fear of movement = Tampa scale for kinesiophobia (TSK) is a 17 item scale to assess the fear of re-injury due to movement. Identification of personal and environmental factors provides the opportunity to incorporate these elements into treatment strategies with appropriate interventions such activities based on cognitive behavioural strategies. Reducing Pain-Related Fear Peter Lang's bioinformational theory of fear (J Affective Disorders 2000; 61:137-159) predicts to reduce fear - the network mediating the fear needs to be activated - new information needs to be presented to discredit the expectations that are inherent to the fear memory. Demystification of the pain through education, appropriate treatment with graded exposure which includes operant cognitive behavioural activity parameters are the cornerstone of such an approach. Paradoxically, verbal re-assurance may have the opposite affect and lead to increased distress. Neurolinguistic programming and Cognitive Behavioural Therapy should be incorporated into the overall management approach
Non specific low back pain The 5th international congress in low back pain concluded last week in Melbourne (Nov 2004). Apart from the usual palabra, there seemed to be some common sense coming from the floor into the discussions. The great proponents of reductionist paradigms for studying so called 'non-specific low back pain' came under fire for the 10 years of misdirected and misguided research trying to identify specific variables using a non-specific paradigm. Cognitive factors, including beliefs, depression, kinesiophobia were thought to make up around 50% of measurable outcome variables, disability 30% and impairment only 20%. Whilst the statistical methodology & reasoning was highly commendable, the premise of a lot of research on the efficacy of treatment interventions was that all physiotherapists are equal. It would seem ludicrous that the same proponents of graduate programmes in Musculoskeletal and Sports Physiotherapy can rationalise that the skill level of the physiotherapist is irrelevant to outcome. These arguments seem to have arisen from poorly designed investigations in the mid 90's. Impairment measures are traditionally seen as 'range of movement' and sometimes neurological impairment. However, more difficult measures which usually aren't included in impairment measures are quality of movement, and the muscle activation required for the distribution of force across joints and between body segments ( inverse dynamics and Newtons 3rd Law). Additionally, when considering the 'mass-spring' analogy of movement and energy conservation, then perturbations of movement and the capture of energy from perturbations of movement, such as plyometrics , become important aspects in the clinical reasoning paradigm. Yet, how are these measured in the NSLBP paradigm by traditional 'non-progressive' research. Those same protagonists also argued in the 1990's that there was no role for dose in manual therapy. (Dose representing the force, duration, frequency, number of repetitions, the type of technique used commiserate with the stage, stability, severity and irritability of the disorder as well as based on the identification of the 'cause of the cause' of the dysfunction). Additionally, back in the 1990's they used placebo constructs which ignored the fundamental role of higher centres in pain and information processing. Even the paper which I submitted to Manual Therapy for publication in the mid 90's on mechanical traction had the descending modulation and cortical modulation aspects deleted from it by the co-authors. Thankfully, multi-modal treatment approaches are now receiving some credibility as a research paradigm. Additionally, the biomechanics and specific treatment intervention for pelvic girdle dysfunction is being extracted out of the NSLBP paradigm. Progressive research on impairment and specifically the importance of muscular forces are being performed by Wim Dankearts under the guidance of Peter O'Sullivan. They are working towards a novel classification system for non specific chronic low back pain patients which includes higher order mental processing. Specifically, Peter O'Sullivan has put forward 3 sub-categories
(5th Interdisciplinary World Congress on Low Back and Pelvic Pain, Melbourne, 2004, Australia p132) |
|
|
This email address is being protected from spambots. You need JavaScript enabled to view it. |
|


Updated : 29 September 2012
 What We do
What We do What We Treat
What We Treat



















































































































