



Active Leg Extension
- Active Hip Extension test involves the client prone and extending their straight leg at the hip. Frequently, clients with LBP and PGP present with reversed gluteal : hamstring timing whereby the hamstrings are dominant. The addition of compression anteriorly or posteriorly can glean information w.r.t force closure. A positve result would be improved timing of contraction of the Gluteus Maximus over the hamstrings. Additionally, a reduction in pain and/or the movement feeling easier 'lighter' to do may also occur. Takasaki et al (Manual Therapy, 2009, 14, 484-489) found that the addition of 50N and 100N anterior compression resulted in the gluteus maximus coming on sooner (263+-99.5ms vs 183.5+-77.9ms vs 91.5+-49.7ms). Improvements with anterior compression may mean the need for transverse abdominus training. Worsening with anterior compression may mean excessive transverse abdominus contraction. Improvements with posterior compression may indicate the need for deep Multifidus (MF) muscle training. Combinations of anterior and posterior compressionon the ilia resulting in improvements may indicate the need for combined deep MF and Transverse Abdominus training. Compression of the thorax and/or elevation/depression, transverse gliding of specific rib rings can also be used. Palpation for tension in the erector spinae muscles of the L/S and T/S as well as using a 'squeezing technique' around the trigger point of tension may also improve Active Hip/Leg Extension suggesting the need to use techniques (such as relaxation through awareness, trigger point dry needling, fascial release, kinesiotaping, etc) to reduce excessive muscle tension
Therefore ideally, gluteal activation occurs prior to or simultaneously with hamstring activation. Where this does not occur, the therapist should consider
- posterior capsule tightness resulting in anterior translation of the head of femur with gluteal activation (hence reflexogenic inhibition)
- anterior rotation of the ilia (counternutation)
- ischioccocygeus spasms and outflare of the ilia
- neuropathy affecting the gluteal nerves
- excessive psoas major activity
- excessive ribcage tightness and hence sympathetic nervous system activity resulting in firing of the hamstrings (these people will say that no matter how much they stretch they still feel that their muscles are tight)
- intra cortical dyskinesia (see Chronic Low Back Pain for more details)
- ALE and Isometric Latissimus Dorsi testing for force closure :
Active Straight Leg Raise
Do active SLR and check symphysis pubis, then reassess with anterior or posterior ilia compression to ascertain the affect of improved force closure. Reduced pain or easier elevation with anterior compression may be indicative of the need to train the transverse abdominis and horizontal fibres of internal oblique (inner core). Conversely, improvements with posterior compression may be indicative of the need to train the deep multifidus which aids sacral nutation and/or train the muscles and fascia of the posterior outer sling.
Do active straight leg raise (ASLR) with or without anterior or posterior compression of the ilia to ascertain 'force closure'. Combinations of anterior and posterior compression on opposite sides is also extremely useful where a sacral torsion is involved. Improvements with anterior compression may mean the need for transverse abdominus training. Worsening with anterior compression may mean excessive transverse abdominus contraction. Improvements with posterior compression may indicate the need for deep Multifidus muscle training. Combinations of anterior and posterior compression resulting in improvements may indicate the need for combined deep MF and Transverse Abdominus training.
The effects of manual pelvic compression on trunk motor control during an active straight leg raise in chronic pelvic girdle pain subjects.
Beales DJ, O'Sullivan PB, Briffa NK. Man Ther. 2010 Apr;15(2):190-9. Epub 2009 Nov 28.
A sub-group of pelvic girdle pain (PGP) patients with a positive active straight leg raise (ASLR) responds positively to the application of external pelvic compression during the test. This study investigated the effect of this phenomenon on electromyographic (EMG) activity of the trunk muscles and intra-abdominal and intra-thoracic pressures in subjects with a unilateral sacroiliac joint (SIJ) pain disorder (n=12). All subjects reported reduced difficulty ratings during an ASLR with pelvic compression (paired t-test: p<0.001), yet no statistically significant changes in the muscle activation or pressure variables were found. However, visual inspection of the data revealed two divergent motor control strategies with the addition of compression. Seven subjects displayed characteristics of a decreased EMG profile, while in the other five subjects the EMG profile appeared to increase. As such this study provides preliminary evidence of two disparate patterns of motor control in response to the addition of pelvic compression to an ASLR. The findings may reflect different mechanisms, not only in the response to pelvic compression, but also of the underlying PGP disorder.Additionally, pressure through the thorax and/or leveation/depression/transverse gliding of specific rib rings can be quite useful to ascertain the influence of rib malalignment and minor instability on ALSR. This again gives immediate diagnostic relevance as well as giving immediate awareness to the client of the existence of a problem.
Compressor Belts for the pelvis may also be useful for some people, however they should only be seen as a means to an end i.e. allow the possibility to function..
The use of pressure through the thorax and ilia can be also be used whilst assessing the clients specific relevant movement problem.
Altered motor control strategies in subjects with sacroiliac joint pain during the active straight-leg-raise test.
O'Sullivan PB, Beales DJ, Beetham JA, Cripps J, Graf F, Lin IB, Tucker B, Avery A., Spine (Phila Pa 1976). 2002 Jan 1;27(1):E1-8.
STUDY DESIGN: An experimental study of respiratory function and kinematics of the diaphragm and pelvic floor in subjects with a clinical diagnosis of sacroiliac joint pain and in a comparable pain-free subject group was conducted.OBJECTIVE: To gain insight into the motor control strategies of subjects with sacroiliac joint pain and the resultant effect on breathing pattern.
SUMMARY OF BACKGROUND DATA: The active straight-leg-raise test has been proposed as a clinical test for the assessment of load transfer through the pelvis. Clinical observations show that patients with sacroiliac joint pain have suboptimal motor control strategies and alterations in respiratory function when performing low-load tasks such as an active straight leg raise.
METHODS: In this study, 13 participants with a clinical diagnosis of sacroiliac joint pain and 13 matched control subjects in the supine resting position were tested with the active straight leg raise and the active straight leg raise with manual compression through the ilia. Respiratory patterns were recorded using spirometry, and minute ventilation was calculated. Diaphragmatic excursion and pelvic floor descent were measured using ultrasonography.
RESULTS: The participants with sacroiliac joint pain exhibited increased minute ventilation, decreased diaphragmatic excursion, and increased pelvic floor descent, as compared with pain-free subjects. Considerable variation was observed in respiratory patterns. Enhancement of pelvis stability via manual compression through the ilia reversed these differences.
CONCLUSIONS: The study findings formally identified altered motor control strategies and alterations of respiratory function in subjects with sacroiliac joint pain. The changes observed appear to represent a compensatory strategy of the neuromuscular system to enhance force closure of the pelvis where stability has been compromised by injury.
Motor control patterns during an active straight leg raise in chronic pelvic girdle pain subjects.
Beales DJ, O'Sullivan PB, Briffa NK. Spine (Phila Pa 1976). 2009 Apr 20;34(9):861-70.
STUDY DESIGN: Repeated measures.
OBJECTIVE: To investigate motor control (MC) patterns in chronic pelvic girdle pain (PGP) subjects during an active straight leg raise (ASLR).
SUMMARY OF BACKGROUND DATA: The ASLR is a test used to assess load transference through the pelvis. Altered MC patterns have been reported in subjects with chronic PGP during this test. These patterns may impede efficient load transfer, while having the potential to impinge on respiratory function and/or to adversely affect the control of continence.
METHODS: Twelve female subjects with chronic PGP were examined. Electromyography of the anterior abdominal wall, right chest wall and the scalene, intraabdominal pressure, intrathoracic pressure, respiratory rate, pelvic floor kinematics, and downward leg pressure of the nonlifted leg were compared between an ASLR lifting the leg on the affected side of the body versus the nonaffected side.
RESULTS: Performing an ASLR lifting the leg on the affected side of the body resulted in a predominant MC pattern of bracing through the abdominal wall and the chest wall. This was associated with increased baseline shift in intraabdominal pressure and depression of the pelvic floor when compared with an ASLR lifting the leg on the nonaffected side.
CONCLUSION: This MC pattern, identified during an ASLR on the affected side of the body, has the potential to be a primary mechanism driving ongoing pain and disability in chronic PGP subjects.
The effect of increased physical load during an active striaght leg raise in pain free subjects.
Beales DJ, O'Sullivan PB, Briffa NK. J Electromyogr Kinesiol. 2010 Aug;20(4):710-8. Epub 2010 Jan 20.
PURPOSE: It has been proposed that pelvic girdle pain (PGP) subjects adopt a high load motor control strategy during the low load task of the active straight leg raise (ASLR). This study investigated this premise by observing the motor control patterns adopted by pain free subjects during a loaded ASLR (ASLR+PL).METHOD: Trunk muscle activation, intra-abdominal pressure, intra-thoracic pressure, pelvic floor motion, downward pressure of the non-lifted leg and respiratory rate were compared between resting supine, ASLR and ASLR+PL. Additionally, side-to-side comparisons were performed for ASLR+PL.
RESULTS: Incremental increases in muscle activation were observed from resting supine to ASLR to ASLR+PL. During the ASLR+PL there was a simultaneous increase in intra-abdominal pressure with a decrease in intra-thoracic pressure, while respiratory fluctuation of these variables were maintained. The ASLR+PL also resulted in increased pelvic floor descent and greater downward pressure of the non-lifted leg. Trunk muscle activation was comparable between sides during ASLR+PL in all muscles except lower obliquus internus abdominis, which was more active on the leg lift side.
CONCLUSION: Pain free subjects respond to an ASLR+PL by a general increase in anterior trunk muscle activation, but preserve the pattern of greater activation on the side of the leg lift observed during an unloaded ASLR. This contrasts to findings in PGP subjects who, despite having a high load strategy for performing an ASLR on the symptomatic side of the body, display equal bilateral activation of the anterior abdominal wall during the ASLR. This differentiates PGP subjects from pain free subjects, supporting the notion that PGP subjects have aberrant motor control patterns during an ASLR.
Changes in pelvic floor and diaphragm kinematics and respiratory patterns in subjects with sacroiliac joint pain following a motor learning intervention: a case series
O'Sullivan PB, Beales DJ. Man Ther. 2007 Aug;12(3):209-18. Epub 2006 Aug 17.
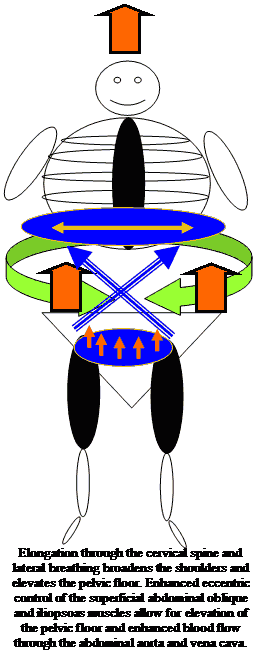
This study was a case series design. The objectives of the study were to investigate the ability of a motor learning intervention to change aberrant pelvic floor and diaphragm kinematics and respiratory patterns observed in subjects with sacroiliac joint pain (SIJP) during the active straight leg raise (ASLR) test. The ASLR test is a valid and reliable tool to assist in the assessment of load transference through the pelvis. Irregular respiratory patterns, decreased diaphragmatic excursion and descent of the pelvic floor have been reported in subjects with SIJP during this test. To date the ability to alter these patterns has not been determined. Respiratory patterns, kinematics of the diaphragm and pelvic floor during the ASLR test and the ability to consciously elevate the pelvic floor in conjunction with changes in pain and disability levels were assessed in nine subjects with a clinical diagnosis of SIJP. Each subject then undertook an individualized motor learning intervention. The initial variables were then reassessed. Results showed that abnormal kinematics of the diaphragm and pelvic floor during the ASLR improved following intervention. Respiratory patterns were also influenced in a positive manner. An inability to consciously elevate the pelvic floor pre-treatment was reversed. These changes were associated with improvement in pain and disability scores. This study provides preliminary evidence that aberrant motor control strategies in subjects with SIJP during the ASLR can be enhanced with a motor learning intervention. Positive changes in motor control were associated with improvements in pain and disability. Randomized controlled research is required to validate these results.Alexander Technique for Lumbopelvic, Thoracolumbar and Scapulothoracic support through elongation of the Upper Cervical Spine
www.back-in-business-physiotherapy.com
Updated : 22 December 2012

 What We do
What We do What We Treat
What We Treat



















































































































