



Case Study of a man with pelvic floor pain from pudendal nerve entrapment
A 36year old male patient presented with low back pain and associated buttock, groin and lateral thigh pain. He also had pins & needles, redness and swelling in the groin. It was aggravated by sitting for longer than 2hours, driving a car and playing golf. It was eased by standing, walking or with the use of Tramidol. It had a gradual and insideous onset two months previously. He saw his local GP who witnessed the rash, and perscribed a single course of anti-biotics. He holidayed for one month, when the conditioned worsed, possibly due to prolonged sitting on a plane. He returned to the GP, who perscribed a further course of anti-biotics and referred to a urlologist for further investigation. He had no history of low back pain, but had some testicular swelling in the past. He had a Lumbar X-Ray, which was clear. He played golf twice per week, and attended the gym four times per week to perform weights and cardio exercises with no complaints.
Clinical history
On initial physical assessment, he had some pain on active lumbar extension and left lateral flexion. His left straight leg raise was very limited to 40degrees by pain, and his gluts were very tight bilaterally. He otherwise had good lumbar and hip range of motion. Treatment included lumbar spine facet joint mobilisations, soft tissue release to his gluts and QL, and a home exercise program to include sciatic nerve glides, glut and lumbar rotation stretches. Immediately after treatment he had full and pain free lumbar extension, and full left lateral flexion, but with some pain. At his second appointment, he reported significant improvements to his pins & needles, and had a decrease in his lateral thigh pain. He felt better after the treatment, and improved overall. It was at the second appointment that the patient mentioned another symptom of erectile dysfunction. A similar treatment was performed with further decreases immediately after treatment. At the third treatment, he reported that there had been no further benefit after the second treatment. On further physical examination, it was found that his left straight leg raise had improved to 70degrees with no pain and equal to the right side. However, he did have some tightness in his ITB and TFL. He found the pain varied with the use of Tramidol. Soft tissue release to his ITB and TFL made his gait easier, and stretches for his ITB were added to the exercises he was already doing. At the forth treatment, he reported significant improvements with decreasing pain, decreasing rash and possible improvements in errectile function. He had full and pain free lumbar range of motion, normal straight leg raise. A repeat treatment from his thrid session was done to good effect immediately after treatment. Over sessions five, six, seven and eight, he continued to report improvements, to the point of having no referred symptoms into his legs, no rash, and no pins & needles. He still had some low back and buttock pain, but it was decreased by 30% overall. His errectile dysfunction persisted. His pain medication had reduced to one neurofen per day and Tramidol three times per week. Further treatment included postural advice for sitting, taping, lumbar and sacro-iliac joint mobilisations, and soft tissue massage. Further exercises were added to include hip rotator and adductor strengthening. At session nine, and after limited improvements to his low back pain and errectile dysfunction, despite being diligent in attending physiotherapy and performing the exercises, he was further encouraged to see a second GP, which he did. He had a CT scan of his lumbar spine, which was clear.
Eighteen months later, the patient reported that further MRI scans of his lumbar spine were clear. He did report being improved with physiotherapy, however he still had some low back pain after prolonged sitting for more than 2hours, and errectile dysfunction. He eventually was refered to Prof Vancaille of WHRIA, who had a specific MRI performed, which concluded he had a Prudendal Nerve Root entrapment. Surgery for this condition has been scheduled for the near future. Pudendal Nerve entrapment was originally described in 1987, and a systematice review by Stav et al in 2009 described the prevalence Pudendal Nerve Entrapment as “unknown and it seems to be a rare event.” Another Literature review by Santos et al in 2010 reported that patients with Pudendal Nerve Entrapment visited between ten and thirty doctors, and waited an average of four years (ranging between one and fifteen years) before diagnosis was made.
Pathomechanics
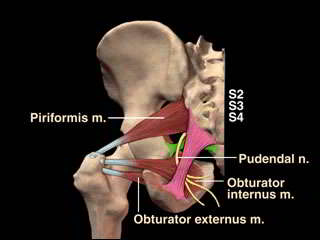
It has been hypothesised that hypertrophy of the muscles of the pelvic floor during the years of youthful athleticism causes elongation and posterior remodeling of the ischial spine. The sacrospinous ligament then rotates, causing the sacrotuberal (ST) and sacrospinal (SSp) ligaments to overlie one another. The ligaments act as a tornique, in what is referred to as Alcock's canal, with the pudendal nerve traversing the interligamentous space where it can be crushed. In this course it may stretch over the SSp ligament or the ischial spine during squatting or during sitting or standing from a seated position. It has been surmised that the gluteus muscle, intimately attached to the ST ligament, exerts a shearing effect as it extends the hip while the pelvic floor is forced inferiorly during the Valsalva maneuver (Stanley J. Antolak, Jr., M.D., David M. Hough, M.D., Wojciech Pawlina, M.D., Robert J. Spinner, M.D. 2013).
Additional explanations include posterior pelvic floor muscle overactivity affecting the ischiococcygeous, piriformis and obturator internus muscles creating a narrowing interfacing with Alcock's canal.
Anatomy
 Innervation
Innervation
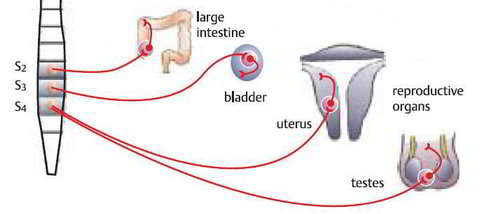
The Pudendal Nerve arises from the nerve roots S2, S3 and S4, so it shares some nerve roots with the Sciatic Nerve. It consists of 80% sensory fibres and 20% motor fibres. It has three branches.The inferior rectal nerve supplies the anal canal, peri-anal skin, rectum and external anal sphincter. The perineal nerve supplies the perineum, vagina, urethra,male scrotum, labia, transverse perineal muscle and urethral sphincter. The dorsal nerve of the clitoris or penis supplies the skin of the clitoris/penis, bulbocavernous, and ischiocavernosus muscles.
Differential diagnosis
Differential diagnosis using an MRI for a Tarlov's cyst should be carried out. In 2005, I saw 2 clients with Tarlov's cysts in the lumbar spine, thoracic and sacral regions, who presented with some low back pain but predominantly claudication type symptoms (generalised leg symptoms including 'ants crawling' & 'spider crawling') as well as some abdominal bloating. I had seen each of them some time previously for an episode of low back pain. Both had successful surgical intervention.
Tarlov cysts are fluid-filled nerve root cysts found most commonly at the sacral level of the spine – the vertebrae at the base of the spine. These cysts typically occur along the posterior nerve roots. Cysts can be valved or nonvalved. The main feature that distinguishes Tarlov cysts from other spinal lesions is the presence of spinal nerve root fibers within the cyst wall, or in the cyst cavity itself.
Due to the close proximity to the lower pelvic region, patients may be misdiagnosed with herniated lumbar discs, arachnoiditis, and in females, gynecological conditions. An accurate diagnosis may be further complicated if the patient has another condition that affects the same region.
Incidence and Prevalence
Small, asymptomatic Tarlov cysts are actually present in an estimated 5 to 9 percent of the general population. However, large cysts that cause symptoms are relatively rare. Tarlov cysts were first identified in 1938, yet there is still very limited scientific knowledge available.
In a recent Tarlov cyst survey, an estimated 86.6 percent of respondents were female, and 13.4 percent were male. This condition affects women far more frequently than it affects men. The largest majority of respondents were ages 31 to 60, with a combined total of 80.4 percent in that age demographic.
An estimated 33 percent of respondents had a cyst(s) present in other parts of the body, most commonly the abdomen or hand and wrists.
An estimated 3 percent of respondents had no pain; 4.2 percent categorized their pain as very mild; 7.6 percent as mild; 31.5 percent as moderate; 38.6 percent as severe; and 15.1 percent as very severe.
Source: Tarlov Cyst Support Group, Tarlov Cyst Survey
Causes
Although the exact cause is unknown, there are theories as to what may cause an asymptomatic Tarlov cyst to produce symptoms. In several documented cases, accidents or falls involving the tailbone area of the spine caused previously undiagnosed Tarlov cysts to flare up.
Symptoms
An increase in pressure in or on the cysts may increase symptoms and cause nerve damage. Sitting, standing, walking, and bending are typically painful, and often, the only position that provides relief, is reclining flat on one’s side. Symptoms vary greatly by patient, and may flare up and then subside. Any of the following may be present in patients that have symptomatic Tarlov cysts.
- Pain in the area of the nerves affected by the cysts, especially the buttocks
- Weakness of muscles
- Difficulty sitting for prolonged periods
- Loss of sensation on the skin
- Loss of reflexes
- Changes in bowel function such as constipation
- Changes in bladder function including increased frequency or incontinence
- Changes in sexual function
Due to the similarity in symptoms between Tarlov's cysts and pudendal nerve injuries it is important to make this differential diagnosis. Additionally, screening questions whose responses indicate cauda equina compression symptoms would require expediation of imaging and specialist consult as serious organ damage may occur.
Cycling
Pudendal nerve injuries are commonly reported in the cycling literature. Specialised saddles for men and women with a gutter in the middle have made some impact on the problem. Additionally, wearing appropriate cycling nicks with padding is equally important.

Treatment
Treatment options endorsed by both the literature reviews of 2009 and 2010, included physiotherapy, pain management medications, cortico-steroid injections and surgery. Physiotherapy can include myofascial release or trigger point releases to the gluteals (minimus, medius and maximus), piriformis, obturator internis, hip adductors, and quadratus lumborum. It can also include neural mobilisations to the sciatic nerve, and dry needling. Muscle energy techniques may also be employed to re-align the pelvis/hip/back complex. There is disagreement in the literature in regards to the effectiveness of stretching and strengthening exercises. In this case, such physiotherapy was partially effective. However, in the end, further surgical management was required in this case.
Decompression surgery is a "last resort", according to surgeons who perform the operation. The surgery is performed by a small number of surgeons in a limited number of countries. The validity of decompression surgery as a treatment and the existence of entrapment as a cause of pelvic pain are highly controversial. While a few doctors will prescribe decompression surgery, most will not. Notably, in February 2003 the European Association of Urology in its Guidelines on Pelvic Pain said that expert centers in Europe have found no cases of PNE and that surgical success is rare:
Pudendal nerve neuropathy is likely to be a probable diagnosis if the pain is unilateral, has a burning quality and is exacerbated by unilateral rectal palpation of the ischial spine, with delayed pudendal motor latency on that side only. However, such cases account for only a small proportion of all those presenting with perineal pain. Proof of diagnosis rests on pain relief following decompression of the nerve in Alcock’s canal and is rarely achieved. The value of the clinical neurophysiological investigations is debatable; some centres in Europe claim that the investigations have great sensitivity, while other centres, which also have a specialized interest in pelvic floor neurophysiology, have not identified any cases.
— European Association of Urology, Guidelines on Chronic Pelvic Pain
Three types of surgery have been done to decompress the pudendal nerve: transperineal, transgluteal, and transichiorectal. A follow-up of patients of this surgery after 4 years found that 50% felt their pain had improved to various extents, although control patients were not followed up for comparison. If surgery does bring relief of symptoms, patients will mostly experience it within 4 weeks of surgery. In this case, email communication from our patient describes significant ability to sit in a painfree manner after surgical interevention.

Conclusion
When making a retrospective analysis it becomes clear, that although many of the symptoms of either cocomittant pathology or secondary hyperalgesia were improving, the underlying pathology around the nerve was not. In fact in the latter stages after he stopped treatment he could only sit for 5 minutes. More emphasis may need to have been placed on the cause of the symptoms - was it an infection which tipped the balance from poor biomechanics to one of pathomechanics? More emphasis should have been placed on the hip musculature as we know that obturator internus myofascia is continuous with the pelvic flooor. Additionally, excessive tension in the adductor muscles would exert an anterior destabilising influence on the hip which in turn can result in counter-nutation and instability of the sacro-iliac joint (SIJ). We also know that the deep hip lateral rotator muscles can play a significant role in the lumbo-pelvic dynamics relating to SIJ dysfunction ('outflares'), as well as infuence the activation pattern of gluteus maximus. As with any pain condition, psychosocial influences need to be taken into consideration, and perhaps even more so in an area of the body associated with sexual function.
Plesae see other sections of this website for information on
- Chronic low back pain
- Muscle energy techniques and sacroiliac dysfunction
- Psychological aspects of musculoskeletal conditions on the immune system
Uploaded : 6 August 2019.
 What We do
What We do What We Treat
What We Treat



















































































































