



Elbow tendinosis/tendonitis/tendinopathy
Tendons are the tissues that attach the muscles to the bones. Overuse in the upper extremities can result in the diagnosis of tendonitis or tendonosis of the wrist, elbow or shoulder. The most common wrist or forearm problems include tendonopathy of the muscles that extend the wrist, otherwise known as tennis elbow. (Ref 3).
The major muscles that move the wrist have thier origin at the elbow. If the wrist is improperly used, pain may arise in the forearm and/or outside elbow. Tennis players and athletes who use a form of backhand, where there is movement in the upper extremities, in repetitive motions that extend and flex the wrist, are particularly at risk. (Ref 1) As the arm muscles are used in this way over and over again, immune and metabolic variables result in the formation of small tears in the tendon leading to irritation, scarring, swelling and lateral elbow pain over time.
Similar to tennis elbow, but less common is golfer's elbow. Pain may be felt on the inside of the elbow and can occur from excessive bending of the wrist toward the palm of the hand. Symptoms may include radiating pain from the inner elbow that extends down the inner forearm, causing weakness of the hand, thumb and wrist. (Ref 1) Patients may experience pain or difficulty when making a fist, shaking another’s hand, and holding, lifting or opening objects. (Ref 1)
Golfer’s elbow, as well as tennis elbow, may not only affect the individual who participates in this type of sport, but could also cause pain in patients who use a screwdriver or hammer on a daily basis or those who spend a great amount of time gardening, raking, or painting. Patients may experience a painful burning sensation if they are excessively turning the wrist, working daily with bent hands at the computer, sleeping with wrists in a curled position, or apply any sustained direct pressure to the area.
Treatment of tendonopathy will depend on which tendon in the arm has been injured. Painful episodes may only last for a few days or can cause ongoing pain that is persistent over several weeks, or even months. The options of many are a home program which may utilize arnica cream, an ice pack along with the support of an adhesive tape or brace at the elbow or wrist. Patients who ice the wrist or elbow area may find temporary relief from pain and swelling, however it’s important not to place ice directly on the skin to avoid a cold burn.
Further treatment for patients with regular elbow pain and wrist conditions include physiotherapy for preventative and long-term improvement of the injury. Physiotherapy massage, dry needling, myofascial massage, ultrasound and joint manipulation can aid in recovery and overall function of the wrist, elbow, and forearm areas. Techniques may also include specific eccentric stretching exercises, in conjunction with a sustained ‘mobilisations with movement’ (MWM), to strengthen the tendon and other surrounding muscles to help regain normal use of the arm and hand. The cervical and thoracic spines may also need treatment for neural irritation which is creating referred pain and neurogenic inflammation and weakness around the shoulder and elbow. Additionally, exercises called neural mobilisations, in the form of ‘sliders and gliders’, can be employed, to improve the health of the radial and ulnar nerves.
Clinical reasoning in determining the nature of elbow pain
Tennis elbow is the common nomenclature for lateral (outside) elbow pain, whereas medial (inside) elbow pain is referred to as Golfers elbow. Traditionally, both conditions have been attributed to tendonopathy. However, both pathologies can be as a consequence of malaligned bones in the elbow and/or carpals, tendonopathies, capsular pain, radial and ulnar nerve pain (Tennis and Golfers elbow respectively), neck and thorax dysfunction. The following outlines the process of clinical reasoning and uses a case presentation to illustrate how an uncommon cause of elbow pain can be discovered using this form of structured cognitive reasoning.

The examination process and the correlation of findings.
It is the job of the physiotherapist to use a systematic approach to assessment to come to terms of the nature and characteristics of the pain. The correlation of various 'signs and symptoms' allow for the establishment of a robust diagnosis.
Frequently, tennis elbow is treated with soft tissue massage, ultrasound and some stretches. However, there are several reasons which need to be addressed when ascertaining what has lead to the onset of tennis elbow. These reasons are usually highlighted in the clients response to questioning during the subjective examination which are subsequently clarified by manual therapy testing in the physical examination. In such a manner an holistic, patient centred, approach is taken to treat a condition which could become severe and disabling if treated inadequately. Importantly, the aim of the physiotherapist is not to treat every single structure and hope for the best. Rather, the physiotherapeutic process clarifies the structures which are contributing to the problem. Moreover, the examination defines the order of priority/importance each structure has in the generation of lateral elbow pain.
Mind map of contributing causes of lateral elbow pain
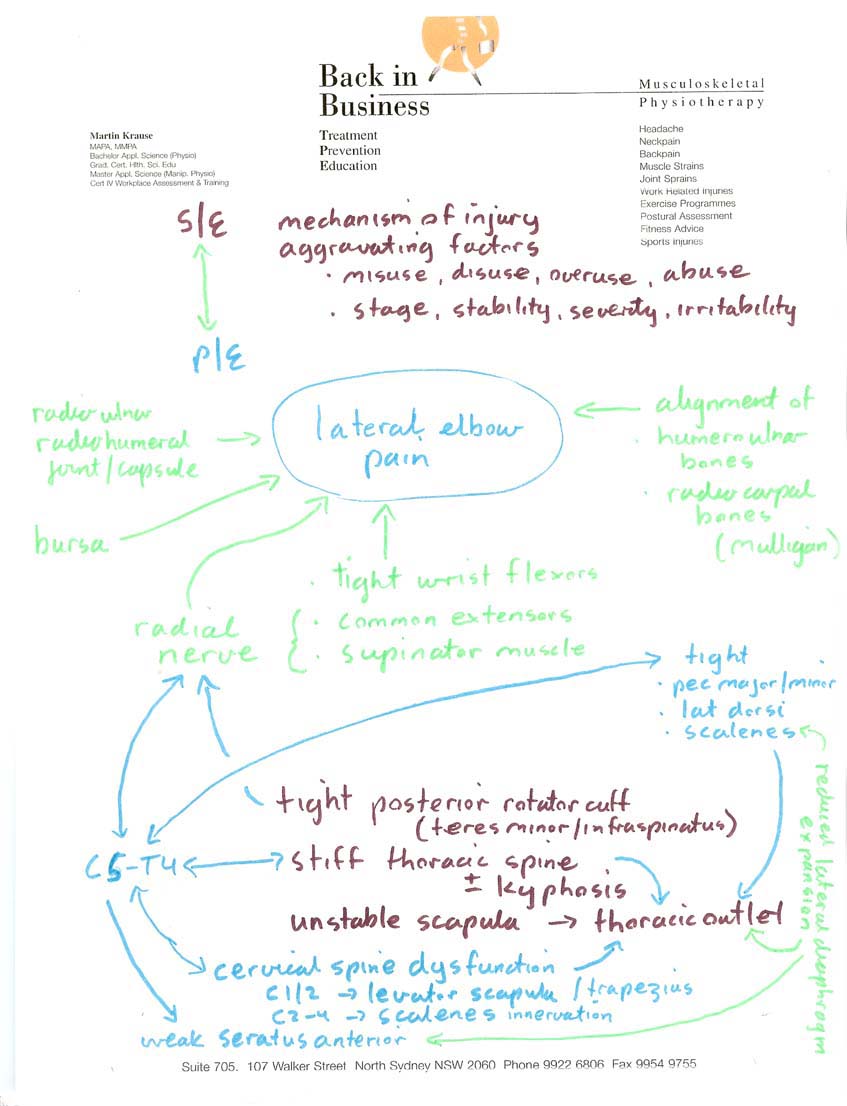
Mind map used for clarifying the multiple possibilties
Refining the mind map into a managable strategy using cognitive filtering
Process for refining the treatment management strategies
Depending on the examination findings, treatment could include
- joint mobilisations to the elbow, cervical and thoracic spines
- soft tissue massage of the scalenes, levator scapula, upper trapezius, latissimus dorsi, wrist flexors
- dry needling of supinator, pronator teres, common extensors, posterior rotator cuff, upper trapezius, thoracic erector spinae
- exercises for scapulo-thoracic-cervical mobility & stability (rhythm)
- exercises for thoracic (vertebrae & ribs) mobility and cervical mobility & stability
- mobilisation with movement (MWM's - Mulligan's technique) for upper ribs, wrist and elbow
- Mulligan's and/or McConnell's taping
- Kinesiotaping
- prescription of elbow or wrist brace
- strengthening exercises for the shoulder, elbow and wrist
- gentle self massage with arnica of the elbow (5-10 minutes daily), ice or heat, and tennis elbow brace (temporary or during high loading)
Tyler Twist program using a Flexbar
The Tyler Twist program uses the Theraband Flexbar to improve grip strength, pronatation and supination, flexion and extension eccentric strength. It can also be used similarly to a body blade by holding one end and wobbling it.


Case presentation of a person with lateral elbow pain
Clearly, in this scenario, the "typical tennis elbow" with mid finger extension pain and ball sqeezing pain, had atypical medial elbow nerve pain, an anteriorly subluxating shoulder and some significant neck-scapula-thoracic spine dysfunction. The process of the physical examination clarified the significance of the limited information given during the subjective examination.
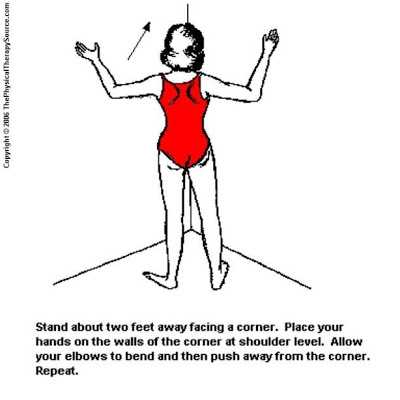
In the corner push-ups can be used as an anterior stabiliser of the shoulder, de-activator of the posterior rotator cuff and act as a scapular mobiliser on the ribcage whilst creating a minimal load on the elbow.
Exercises for stretching and strengthening the posterior capsule of the shoulder and stretching the forearm flexors (not extensors)
Anatomical validity in treating the neck for shoulder - shoulder blade dysfunctions leading to lateral elbow pain
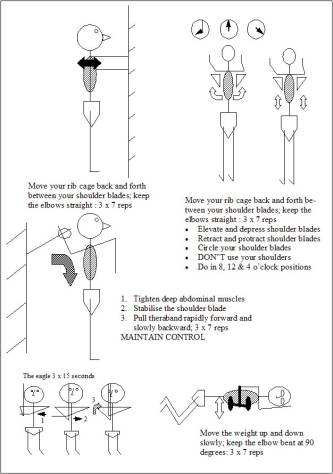
Scapular (shoulder blade) and thoracic stabilisers and mobilisers
Both shoulder and scapula dysfunction needed to be addressed for effectively treating this "tennis elbow".
The role of the diaphragm in thoracic mobility
Thoracic mobility and wrist mobility needed to be addressed. In the thorax the 'rings' need to be 'racked and staked' for optimal sympathetic nervous system tone, which regulates muscle tension and blood flow.
Lateral diaphragmatic breathing had to be taught for scapula dysfunction as well as maintaining normal sympathetic nervous system activity (metabolic acidosis/alkaloses, and sympathetic ganglia rythmical motion)
Posterior shoulder, scapula stabilisation and deep neck flexor exercises
Deep neck flexor training and parascapula-post shoulder training is introduced to reduce upper trapezius tension, thereby reducing the compression loading on the cervical spine, as well as reducing adverse neural tension in the brachial plexus
Self actualisation and combating an existenial clinical crisis through inductive and deductive reasoning incorporating reflective thinking
Clinical reasoning uses cognition & meta-cognition to develop clinical expertise and pratitioner self-actualisation
Video demonstrating Mulligans technique (movement with motion) with an eccentric muscle training program.
Conclusion
The 'typical' lateral elbow pain usually respondes well using a multimodal approach to a potentially multifactorial problem. Addressing, thoracic, cervical, shoulder, wrist and elbow pathology should accelerate recovery whilst reducing the risk of recurrence. Moreover, the clinical reasoning approach readily incorporated an atypical elbow pain due to an unstable shoulder into it's domain, allowing for the design of a unique treatment approach. Successful implementation of a new treatment strategy allows the formation of a new clinical pattern of 'shoulder - elbow pain' Please also see
Motor Learning and shoulder stability
Development of the concepts of stability
Last update :17 October 2017
 What We do
What We do What We Treat
What We Treat



















































































































