



Physiotherapeutic Implications of Functional Clinical Instability in the Lumbar Spine
by Martin Krause
Pathological basis, diagnosis, and conservative management in the clinical reasoning process
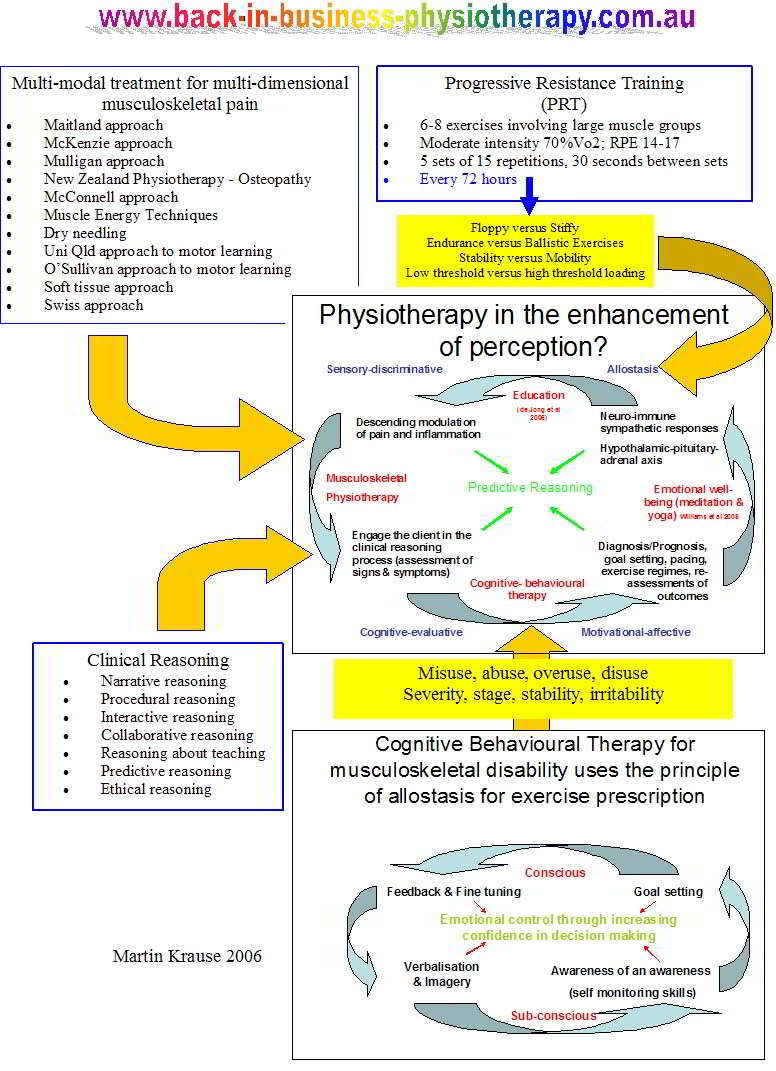
Contemporary approaches to viewing stability create a belief that all control occurs around the neutral zone and hence exercise must be prescribed which maintain the neutral spine. Although this is plausible and potentially true for a structurally unstable spine, and is a useful approach during an acute inflammatory, or seriously splinted by muscle spasm pathology, it is probably a misdirected concept in subacute and chronic pathology. Our rational in the past is to correct what we believe to be incorrect. However, what if the person has a directional preference for recovery? A direction which encourages movement away from the painful pattern rather than towards it. Should this be encouraged to promote blood flow, reduce movement anxiety and engage the dynamic stabilising biomechanics? Afterall, the multifidus has been considered the 'sensor of the spine', yet logic would dictate that it cannot sense any movement, if the spine doesn't move out of it's neutral zone.
Introduction to the stabilizing system
- Passive system comprising the vertebrae, intervertebral discs, zygapophysial joints and ligaments
- The active system comprising the muscles and tendons surrounding and acting on the spinal column
- The neural system comprising the peripheral nerves and central nervous system which direct and control the active system in providing dynamic stability (Panjabi 1992).
Bergmark (1989) hypothesized the presence of two muscle systems that act in the maintenance of spinal stability
- The global system consisting of large torque producing muscles that act on the trunk and spine without directly attaching to it. Tendon to be direction-specific in their stabilising role and therefore produce stability through compression of the vertebrae
- The segmental ‘local’ muscle system consisting of muscles attaching directly to the lumbar vertebrae and are responsible for providing segmental stability and directly controlling the lumbar segments. Tend to be tonically active at low loads and tend to have a multi-directional stabilizing function
Co-ordinated patterns of muscle recruitment are essential between the global and local muscle systems to ensure dynamic stability during activities of daily living (Cholewicki & McGill 1996)
Stabilizing system
The neuromuscular system must provide the necessary compressive forces whilst maintaining the arch like structure of the spine (Aspden 1992)
- The erector spinae and the psoas major are known to significantly increase the compressive load on the lumbar spine (Bogduk 1992) which enhances spinal stiffness and hence stability of the lumbar spine
- The segmental stabilizing role of the multifidus, with separate segmental innervation, acts to maintain the lumbar lordosis and ensure control of individual vertebral segments particularly within the neutral zone (Panjabi et al 1989, Wilke et al 1995). Multifidus also provides proprioceptive information vital for safe functioning of the lumbar spine (Brumagne et al 2000)
- The transverse abdominis and transverse fibres of internal oblique whilst applying some compressive forces to the lumbar spine (McGill & Norman 1987) and pelvis (Richardson et al 2002) are primarily active in providing rotational and lateral stability to the spine via the thoracolumbar fascia while maintaining levels of intra-abdominal pressure (IAP) (Cresswell et al 1992)
- The intra-abdominal pressure mechanism, primarily controlled by the diaphragm, transverse abdominis and pelvic diaphragm also provide an important role in stabilizing the lumbar spine (Aspden 1992, McGill & Norman 1987)
- Pre-activation of the stabilizing muscles provides a base upon which the torque-producing muscles can act safely (Cresswell et al 1994, Hodges & Richardson 1996)
- Inappropriate timing or altered control of these complex mechanisms can result in tissue damage rather than stability to the motion segment (Gardner-Morse et al 1995, McGill & Sharratt 1990)
- Lumbar spine is more vulnerable to instability at low loads (Cholewicki & McGill 1996) and under such conditions only 1-3% MVC may be sufficient to ensure dynamic stability
- During power lifting maintenance of the neutral zone prevents end of range loading tissue strain (McGill & Cholewicki 1992, 2001) through the maintenance of intra abdominal pressure through the co-contraction of loacl and global muscles
Dysfunction of the neuromuscular system
Disruption in the patterns of co-recruitment within and between different muscle synergies (O’Sullivan et al 1997)
- Multifidus and transverse abdominis adversely affected during low back pain (Hides et al 1996), chronic low back pain (Daneels et al 2000) and lumbar instability (Lindgren et al 1993, Sihvonen & Partanen 1990)
- The manner of multifidus dysfunction may vary with different lumbar pathology (Daneels et al 2000; Stokes et al 1992)
- Compensatory substitution strategy to adopt global muscles systems for stabilization with high levels of intra-abdominal pressure (O’Sullivan 2002)
- Changes in the neural control strategy affecting timing of patterns of co-contraction, balance, reflex and righting responses (O’Sullivan et al 1997)
- Generalised changes to trunk musculature such as loss of strength, endurance and muscle atrophy are likely the result of disuse and inactivity, whereas the localised muscle atrophy may be the result of either motor or sensory nerve damage, reflexogenic excitation or inhibition of the muscles proximal to the site of pathology (Stokes et al 1992) and inappropriate mechanoceptive and proprioceptive input, leaving the subject biomechanically vulnerable (O’Sullivan 2005)
Entropy and Low Back Pain
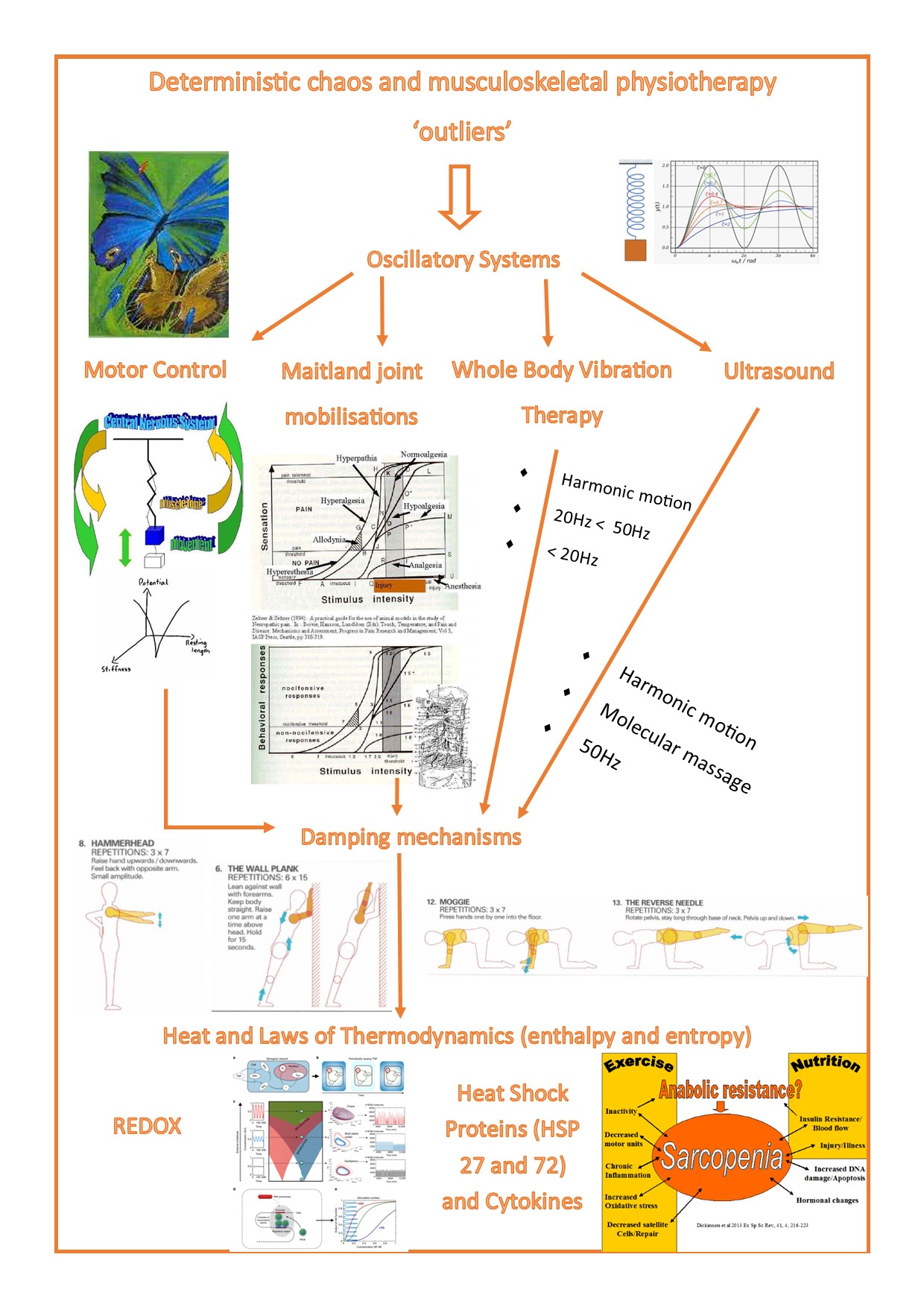
In Musculoskeletal Physiotherapy there has been an emphasis on 'normal'. What is normal function and what are the constraints of a functional movement pattern. Reductionist approaches are taken to ascertain the directions of movement of 'preference' versus those of 'avoidance'. Avoidance in the acute stage of an injury frequently involves 'unloading' the injured area, whereas people with chronically painful movement frequently 'overload' the area of dysfunction. Ironically enough, their movement becomes 'predictable' and less varied. Furthermore, the reduced variability leads to either 'increased control' and less adaptability, or 'reduced control' and increased loading of 'fatiguable structures' (Thiry et al Entropy2022, 24(4), 437; https://doi.org/10.3390/e24040437). Hence, the danger for the physiotherapist is to 'drill' down to the 'offending' structure or movement, but not progress rehabilitation far enough, to include the variety entailed in the full spectrum of complex movement and loading, which is required for motor control in 'predictable' and 'unpredictable' environments. Similar, to the 'Butterfly Effect' in non-linear mathematics, optimisation ultimately requires a chaotic system of control, manifested by 'outliers' which determine the 'damping' or 'amplification' of an oscillating system. Similar, to the 'Butterfly Effect' in non-linear mathematics. Read more : Deterministic Chaos and Musculoskeletal Physiotherapy
Movement based classification of pain disorders
- Mobility of spinal segments in isolation is not predictive or diagnostic in classifying pain disorders
- “It is the association between the mobility and control of the spinal segment, and its relationship to the pain disorder, which appears to be critical” (O’Sullivan 2005)
Peter O'Sullivan has put forward 3 sub-categories
- "Pain disorders associated with movement impairments are associated with a loss of normal physiological movement of lumbo-pelvic mobility, and abnormally high levels of muscle guarding and co-contraction of lumbopelvic muscles with generation of intra-abdominal pressure....[resulting in].....excessive force closure"
- "Pain disorders associated with control impairment are associated with no impairment to the mobility of the symptomatic spinal segment, but rather present with impairments or deficits in control of the symptomatic spinal
segment pressure...[resulting in]....reduced force closure" - "......mal-adaptive movement and motor patterns result in chronic abnormal tissue loading and ongoing pain and distress......These disorders are also invariably associated with non-organic factors but these factors do not dominate the disorder, leaving them more amenable to physiotherapy intervention based on a cognitive behavioural motor learning model" (5th Interdisciplinary World Congress on Low Back and Pelvic Pain, Melbourne, 2004, Australia p132
Clinical instability - functional incompetence
“Clinical instability of a spinal segment represents a loss of functional competence of a spinal segment within its neutral zone of motion with a resulting loading and movement based pain disorder associated with a loss of control” (O’Sullivan 2005)
Pain associated with a functional loss of neutral zone control may manifest in
1. Through range movement pain due to non-physiological motion of the spinal segment
2. Loading based pain due to non-physiological loading of the spinal segment
3. End of range pain or overstrain due to repetitive strain of the spinal motion segment at the end of range (O’Sullivan et al 2003)
One of the problems in the diagnosis of clinical instability lies in the difficulty measuring accurately the functional control of the spinal segment within its neutral zone
Radiological findings only become significant when they can be correlated with clinical findings
50% of people with clinical instability report this to have occurred after a single episode of back pain, whereas the other 50% reported a gradual onset in relation to multiple minor events (O’Sullivan 1997)
Clinical Instability – physical presentation
- Active range of movement reveals good spinal mobility but with aberrant spinal motion associated with a painful arc with or without end range pain (O’Sullivan 1997)
- The aberrant movement is associated with sudden acceleration, hesitation or lateral movement within the mid range of spinal motion
- Segmental hinging of the symptomatic segment is a common feature
- Assistance of movement with the hands is another common feature
- Abolition or significant reduction in pain with the contraction of the transverse abdominis
- Absence of abnormal neurological features (O’Sullivan 1997)
- Confirmation of the abnormality is essential through passive physiological motion testing where flexion/extension and rotation were reported to be most sensitive to detect excessive intersegmental motion.
- For spondylolisthesis and spondylosis excessive motion was detected at the level above the pars defects (O’Sullivan 1997)
- All the physical examination findings have also been reported by Nachemson (1985) and Kirkaldy-Willis 1983), however the sensitivity and specificity and predictive value of these signs are largely unproven (Nachemson 1991; O’Sullivan 2005)
Clinical Instability – neuromuscular examination
- Neuromuscular examination determines the relationship between the motor control of the spinal segment and the pain disorder
- Posture and movement analysis
1. Analysis of aggravating and easing postures and functional movements of the lumbo-pelvic region. Need to determine if there is a strategy of dynamic postural stabilisation and secondly identify whether there is a directional emphasis to the pain disorder
2. Specific movement and postural loading tests dependent upon step 1 and involve tests of spinal proprioception and thoracolumbar control. Here the therapist attempts to correct the posture, movement pattern or specific activation of stabilising muscles then this confirms or negates the notion that motion control affects the pain disorder (O’Sullivan 2005)
3. Specific muscle tests – non functional cognitive tests and therefore lack specificity
– Pelvic floor and transverse abdominal wall (supine, side-lying, sitting)
– Lumbar multifidus with co-contraction of transverse abdominal wall muscles in neutral lordosis (prone, side-lying, four point kneeling, sitting)
– Gluteus maximus (prone)
– Iliopsoas (hip flexion sitting, anterior pelvic rotation in supine and sitting)
– Hip flexor test (Thomas position)
Directional patterns of clinical instability (Peter O'Sullivan)
1. Flexion pattern
– Most common pattern
– Loss of segmental lumbar lordosis at the level of the unstable motion segment. Sometimes noticeable in standing , accentuated in sitting postures with a tendency to hold pelvis in a degree of posterior pelvic tilt.
– Loss of segmental lordosis is accentuated in flexed postures and is usually associated with increased erector spinae tone in the upper lumbar/low thoracic spine with an associated increase in lordosis in the thoracic spine
– Movement into forward bending tends to be initiated at and flex more at the segmental level than at the adjacent levels where there is a tendency to hold the upper lumbar/low thoracic in lordosis, with an associated lack of hip flexion
– Arc of pain into flexion and a tendency to use the hands to return from flexion
– During backward bending there is a tendency to extend above the symptomatic segment
– Inability to anterior pelvic tilt independently of upper lumbar and low thoracic extension
– Jerky staccato movements rather than smooth controlled ones
– Movement tests of squatting, sit to stand, sitting with knee extension and hip flexion reveal an inability to control segmental lordosis and an anterior pelvic tilt position, with a tendency to flex and posterior pelvic tilt instead
– Inability to reposition within the neutral zone and a tendency to over-shoot into flexion
– Inability to activate lumbar multifidus and psoas in co-contraction with the transverse abdominal wall
– Unable to initiate a start position of neutral lumbar spine in 4-point kneeling and sitting, and particular difficulty initiating an anterior pelvic tilt and lordose the low lumbar spine
– Attempts to activate these muscles are commonly associated with Valsalva manoeuvres and bracing of abdominal muscle with loss of breathing control and excessive co-activation of the thoracic erector spinae
2. Lateral shift pattern
– Usually associated with a flexion/lateral shift movement disorder
– In the history commonly complain of an injury into flexion and rotation
– Commonly relate to difficulty reaching and rotating in one direction associated with flexion
– Report relief in extended or lordotic postures
– Report the with minimal precipitation their spine may deviate into a lateral shift position in flexion
– Loss of segmental lumbar lordosis at the affected level with an associated lateral shift
– Atrophy/absence of the lumbar multifidus muscle on the contralateral side to the shift
– Shift is accentuated when standing on the ipsilateral foot of the shift during gait and Stork test
– Tendency to deviate at mid-range flexion and is commonly associated with an arc of pain
– Side bending in the direction of the shift reveals a translatory motion rather than side bending at the unstable level
– Dominant activation of the lumbar multifidus and thoracic erector spinae on the ipsilateral side of the shift and a loss of rotatory and lateral trunk control seen in 4-point kneeling whilst flexing one arm and supine lying lateral leg lowering
– Single leg standing reveals an inability to load the thoracolumbar spine vertically over the pelvis
– Sit-to-standing and squatting reveal a tendency to lateral trunk shift
– Inability to reposition the pelvis with a tendency to overshoot into flexion and lateral deviation
– Attempts to dynamically stabilize the lumbar spine tend to be carried out by dominant activation of the lumbar erector spinae, quadratus lumborum and in some cases the lumbar multifidus on the side of the shift along with the diaphragm and abdominal muscles
3. Active extension pattern
• Lumbar spine is held actively into extension with high levels of concentric muscle activity from the erector spinae and iliopsoas
• Commonly report a single or repetitive extension mechanism of injury, however sometimes they report a flexion incident where they actively fix their spines into extension
• Provocative activities include, standing, erect sitting, forward bending postures (where there is a tendency to hold the lumbar spine in fixed extension), carrying out overhead activities, and an inability to walk fast, run or swim
• Symptoms are relieved in flexion postures such as crook lying in supine
• Segmental hyperlordosis at the unstable level , the pelvis is often in anterior pelvic tilt and the thorax is positioned forward of the pelvis
• Forward bending reveal excessive hip flexion and a tendency to maintain the lumbar hyperlordosis with or without a sudden loss of hyperlordosis at mid-range accompanied by an arc of pain
• Return to neutral accompanied by hyperlordosis and a tendency to need to use the hands
• In sitting there is a tendency to maintain lumbar lordosis and difficulty in posterior pelvic tilting
• Inability to posterior pelvic without the use of hip flexors, rectus abdominis, and external obliques in standing and supine lying
• Hip extension with knee flexion in prone reveals a tendency to hyperextend at the unstable segment with loss of co-contraction of the abdominals and inner range activation of erector spinae and iliopsoas
• Position sense in sitting and 4 point kneeling reveal a tendency to overshoot into extension
• Inability to co-contract segmental lumbar multifidus with transverse abdominal muscles in a neutral lumbar posture, tendency to hyperextend and over-activate segmental extensors, abdominals and inability to control diaphragmatic breathing
4. Passive Extension pattern
• Present with very low tone of the lumbar multifidus, iliopsoas and erector spinae muscles
• Mechanism of injury associated with extension. Similarly aggravating positions involve extension. Flexion positions relieve symptoms
• Unlike the ‘active’ group the ’passive’ group do not report aggravation of symptoms with forward bending activities and postures as they do reverse their lordosis
• Tendency to sway the thorax posterior to their pelvis, with resultant ‘hinging’ of the unstable spinal segment into extension
• This ‘passive’ posture results in deactivation of transverse abdominal muscles, multifidus, gluteals, and erector spinae, with increased tonic activation of the rectus abdominis and external oblique muscles (O’Sullivan 2002)
• In sitting, unlike the ‘active’ group they sit in a slumped posture
• Position sense testing reveals a tendency to overshoot into extension
• Inability to posterior pelvic tilt without dominant activity of the upper abdominal wall and flexion of the thorax
5. Multidirectional pattern
• Most debilitating with high levels of pain,
• Usually of traumatic onset,
• Excessive segmental shifting and hinging patterns may be observed in all movement
directions
Clinical Reasoning
Clearly, there are some movement patterns which are best avoided, as they represent the potential to create neurological compromise. Other patterns to avoid are those which initially were avoided in the acute stage and then later in the subacute phase become the chronic irritating movement pattern. Hence, in those cases the logical argument is to use the directional preference of movement which reduces pain, rather than the inherent movement (motor pattern) which keeps on biomechanically generating more pain.
Oscillating Systems
Oscillating systems are employed by Musculoskeletal Physiotherapists, in many forms, to retrain the movement system, after injury, by improving variability, adaptability to complexity of performance can occur. An wholelistic approach from reductionism to constructivism is undertaken through the various stages of injury and return to sport and activities of daily living.
Uploaded : 13 September 2012
Updated : 9 April 2022
 What We do
What We do What We Treat
What We Treat



















































































































